Case Report

Atypical Radiological Aspect of Intacerebral Tuberculoma: A Case Report and Literature Review
1 Nezha Jalami, 2 Kamal Chtira, 1Nissrine Louhab,3Houssaine Ghannane, 3Said Ait Benali, 1Najib Kissani
- 1.Neurology Department, Arrazi Hospital, University Hospital Mohammed 6, Marrakesh, Morocco
- 2.Neurosurgery Department, Ibn Tofail Hospital, University Hospital Mohammed 6, Marrakesh, Morocco
- 3.Neurosurgery Department, Arrazi Hospital, University Hospital Mohammed 6, Marrakesh, Morocco
- Submitted Monday, September 17, 2018;
- Accepted Thursday, November 1, 2018;
- Published Friday, November 2, 2018
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Introduction:
Cerebral tuberculoma is the most severe form of extra-pulmonary tuberculosis. It is a rare disease representing only 1% of all tuberculosis cases. The authors described a case of cerebral tuberculoma with atypical radiological aspect initially mimicking a tumor lesion.
Case report:
On 12th May 2017, a 28-year-old woman, without a specific antecedent, immunocompetent, was originally addressed for an intracranial hypertension syndrome. On admission the patient was apyretic with a general state preserved. The ophthalmological examination found a papillary edema stage II, and the neurological examination was normal. His first cerebral MRI revealed a cortico-subcortical right occipital lesion with an intense enhancement to the injection of gadolinium, producing a serpiginous appearance; we evoqued on an arteriovenous malformation, reason why a cerebral angiography was requested which was normal. A brain MRI Spectroscopy was made afterwards to look for the nature of the lesion, and the spectroscopic aspect was in favor of a malignant glioma. The diagnosis of glioma has been retained, and the decision of surgical excision is taken. But histological examination of the surgical specimen revealed tuberculosis. The patient was treated with anti-tuberculosis drugs. The CT scan shows an occipital porencephalic cavity, it did not show any new lesions.
Conclusion:
The diagnosis of intracerebral tuberculoma is based on anatomopathological examination. It must be suspected in front of any single brain lesion.
Key words:
intracerebral tuberculoma; atypical; radiological aspect.
Introduction
The tuberculoma is one of the forms of tuberculosis, but it is the most severe and the rarest. It accounts for 1% of all tuberculosis cases. Its incidence varies between 0.5 to 2% of the intracranial masses, in the western countries, and 10 to 30% in the developing countries [1,2]. The intracranial tuberculoma is mostly unique, multiple forms are rare. Its clinical expression depends on the location, number, and size of the lesion. Authors report a case of atypical radiological aspect of intracerebral tuberculoma whose initial aspect is that of a malignant glial tumor.
Case Report
(May 12, 2017, at hospital university Mohammed 6, Marrakesh, Morocco)
This 28 year old female patient, without a specific antecedent, immunocompetent, was originally addressed for an intracranial hypertension syndrome, made of headaches, vomiting, and decreases of visual acuity, evolving since 1 month in a fast progressive way, without fever or deterioration of the general state. On admission the patient was apyretic with a general condition preserved. The ophthalmological examination had founded a papillary edema stage II and the neurological examination was normal. His first cerebral MRI (Figures 1) revealed a cortico-subcortical right occipital lesion with an intense enhancement to the injection of gadolinium, producing a serpiginous appearance; we doubted on an arteriovenous malformation, reason why a cerebral angiography was requested which returned normal.
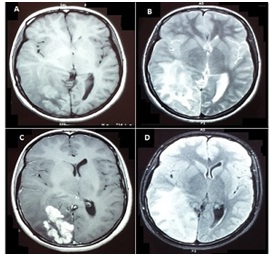

Figure 1: Brain MRI Axial sequences: T1 (A), T2 (B), T1 with Contrast (C) and Flair Sequence (D), showing a right occipital lesional process which appears on isosignal T1 with edema around, hypersignal T2 and T2 flair, it takes the gadolinium intensively realizing a serpeginous aspect, associated with a periesional edema.
A brain MRI Spectroscopy is made afterwards to look for the nature of the lesion, and the spectroscopic aspect was in favor of a malignant glioma (Figures 2). The diagnosis of glioma has been retained, and the decision of surgical excision is taken. After excision of a mass measured 10cm, histological examination highlights edematous and congestive brain tissue, site of tuberculoid granulomatous lesion, with caseous necrosis, without sign of malignancy (Figures 3). The extension assessment did not find any other locations.

Figure 2: Cerebral MR Spectroscopy (MRS) image showing elevated levels of choline and lipids, and reduced NAA

Figure 3: Image of the histological examination with high magnification of the tuberculous granuloma showing the epitheloid granuloma (area surrounded by the black circle). With caseous necrosis (the area surrounded by the red circle).
The patient was treated with anti-tuberculosis drugs, according to the protocol of 2RHZE/7RH. The short-term evolution after surgery was marked by the disappearance of headaches, and vomiting, as well as a clear improvement in visual acuity. The long-term evolution was favorable, on the ophthalmologic plan; the patient did not have visual squeal. Control imaging, CT scan, shows an occipital porencephalic cavity, it did not show any new lesions (Figures 4).

Figure 4: Postoperative CT scan with contrast objectifying an occipital porencephalic cavity
Discussion
Intracranial tuberculoma (ICT) is an avascular granulomatous mass with a necrotic center (casein), which usually measures between 2 and 8 cm, surrounded by normal brain tissue and perilésional edema [3]. In Morocco tuberculosis remains frequent, and is a public health problem. Its emergence has been observed since the AIDS pandemic [4], The latter is considered to be one of the main risk factors for tuberculosis, But it could be seen in an immunocompetent patient [5,6], as was the case with our patient. Its clinical expression is extremely varied, depending on the size and location of lesions. The beginning is progressive by appearance of an alteration of the general state. Clinical data, although not specific, include signs of intracranial hypertension, neurological deficit, convulsive seizures, cerebellar syndrome, meningeal syndrome, visual disturbances. Fever is observed only in 10 to 15% of cases [2-7].
Delay of diagnosis is varied, depending on the clinical signs, and the socio-economic level. In a retrospective study of 125 cases; the average diagnosis delay was 6 months (3 weeks-4years) [4], in our case it was 1 month. However, cases of completely asymptomatic cerebral tuberculomas have also been reported [8, 9]. The appearance of tuberculomas at CT scan and MRI depends on the evolutionary stage of necrosis. In MRI, non-caseated tuberculomas appear to be hypo intense T1 and hyper signal T2 in relation to the cerebral parenchyma, and are enhanced in an intense and homogeneous manner by the contrast agent. Caseated tuberculomas with a solid center appear in hypo or isosignal T1 and in hypo or isosignal T2 and often associated with perilesional edema. While the tuberculomas casenetized with necrotic center appear in hypo signal T1, and hyper signal T2, and are elevated at the periphery by the product of contrast. Tuberculomas present on the T1 sequences without injection a peripheral T1 hypersignal borderline, specific for tuberculosis [10,11,12]. In a retrospective study of 1247 cases of ICT, half of them were located in the parietal lobes [13]. Whereas, in our patient, the lesion was in the left occipital lobe. The absence of other localizations of tuberculosis and the radiological aspect made it more difficult to diagnose the disease in our patient, especially since there was no associated fever.
From a therapeutic point of view, all authors confirm the efficacy of anti-bacillaries in the absence of resistance [14].The use of surgery is rarely justified, given the documented efficacy of antituberculosis drugs. However, surgery may be necessary, either in cases of intracranial hypertension or after failure of the anti-tuberculosis test, or in case of doubt about the diagnosis [14]. As for the case of our patient, a surgical intervention was rapidly performed, due to the involvement of the visual prognosis and also for a diagnostic purpose.
In the African series, the neurological sequelae varies from 33.3 to 37.5%, this rate is closely correlated with age of patient, the delay of diagnosis, and time to initiation of anti-tuberculosis drugs, and the presence or not of neurological disorders [6]. In our case, there were no visual or neurological sequelae.
Conclusion
The diagnosis of intracerebral tuberculoma is based on anatomopathological examination confirmation, and imaging does not often make it possible easy to evoke tuberculoma. The search for tuberculosis localization must be systematic. We believe that in developing countries as like ours, or at risk individuals, tuberculoma should be suspected in front of any single brain lesion. Its prognosis depends closely on the early diagnosis and the rapidity of therapeutic management.
Ethical Consideration
The written consent was issued to the author by the patient for the publication of his case for a scientific purpose by deleting the patient's identity from the figures of manuscript.
Conflict of Interest
All authors declare that they have no conflict of interest
Author's Contribution
1. Chtira Kamla, Nezha Jalami, Nissrine Louhab: the idea design, and article writing, and participation in patient management.
2. Houssaine Ghannane,Said Ait Benali: The critical reading of the article.
3. Najib Kissani: Final correction and verification of scientific data of the article.
Acknowledgements
1. To all the medical and nursing staff of the neurosurgery department of the Ibn Tofail Hospital, and Arrazi Hospital of the university hospital Mohammed 6- marrakesh-Morocco.
2. To all the medical and nursing staff of the Neurology department o Arrazi hospital of the university hospital Mohammed 6- marrakesh-Morocco.
References
[1].Shah IA, Asimi RP, Kawoos Y, Wani M, Sarmast AH. Tuberculomas of the Brain with and without Associated Meningitis: A Cohort of 28 Cases Treated with Anti-Tuberculosis Drugs at a Tertiary Care Centre. Journal of Contemporary Medical Research. 2016;3(12):3484-7. https://www.ijcmr.com/uploads/7/7/4/6/77464738/ijcmr_1131_jan_6.pdf
[2].Nicolls DJ, King M, Holland D, Bala J, del Rio C. Intracranial tuberculomas developing while on therapy for pulmonary tuberculosis. The Lancet Infectious Diseases. 2005 ;5(12):795 801[PubMed]
[3].Mazza-Stalder J, Nicod L, Janssens JP. La tuberculose extrapulmonaire. Revue des maladies respiratoires 2012; 29(4): 566-78.[pubmed]
[4].Moufid F, Oulali N, El Fatemi N, Gana R, Maaqili R, Bellakhdar F. Les tuberculomes intracraniens: à propos de 125 cas. Pan African Medical Journal. 2012;12(1):56.[pubMed]
[5].Vidal JE, Hernández AV, Oliveira AC, Souza AD, Madalosso G, Silva PR, Dauar R. Cerebral tuberculomas in AIDS patients: a forgotten diagnosis?. Arquivos de neuro-psiquiatria. 2004; 62(3-B):793-6[PubMed]
[6]Adeolu AA, Shokunbi MT, Malomo AO, Akang EA, Obajimi MO, Komolafe EO. Solitary intracranial tuberculoma in patients without immuno-suppression: a report of three cases. The Nigerian postgraduate medical journal. 2006 ;13(1):69-72.[PubMed]
[7].El-Sayed MM, Adeuja AO. Intracranial tuberculomas: the Hofuf, Saudi Arabia experience. African journal of medicine and medical sciences. 2006;35(1):21-7.[PubMed]
[8].Bazin C. Tuberculose du système nerveux central. EMC-Neurologie. 2004 ;1(2):169-92. https://doi.org/10.1016/j.emcn.2003.12.003
[9].Laghmari M, Thouassa G, Mpando D, Benali SA. Tuberculosis of the Nervous System in Immunocompromised Hosts. InTuberculosis of the Central Nervous System, Springer, Cham.2017.p.499-509. https://link.springer.com/chapter/10.1007/978-3-319-50712-5_35
[10].Bleibtreu A, Grall N, Laissy JP, Rioux C, Strukov A, Lariven S, Yeni P, Yazdanpanah Y, Joly V. Contribution of brain imaging to the diagnosis of intracranial tuberculoma and other brain lesions in patients presenting with miliary tuberculosis. Med Mal Infect (2017).[PubMed]
[11].Kim JK, Jung TY, Lee KH, Kim SK. Radiological follow-up of a cerebral tuberculoma with a paradoxical response mimicking a brain tumor. J Korean Neurosurg Soc 2015;57:307–10.[PubMed][Free PMC Article]
[12].Krishnan V, Mittal MK, Sinha M, Kumar M, Thukral BB. Central nervous system tuberculosis: Rare presentations of a common disease. Astrocyte. 2017;4:174-85. http://www.astrocyte.in/text.asp?2017/4/3/174/224198
[13].Chin JH, Mateen FJ. Central nervous system tuberculosis: challenges and advances in diagnosis and treatment. Current infectious disease reports. https://doi.org/10.1007/s11908-013-0385-6
[14].Katti MK. Pathogenesis, diagnosis, treatment, and outcome aspects of cerebral tuberculosis. Medical Science Monitor. 2004;10(9):RA215-29.[PubMed]

