Original Article

Intraoperative ultrasound guided spinal tumor resection
Deepak Patil, Vivek Sharma, Divye Prakash Tiwari
Department of Neurosurgery, Institute of Medical Sciences, BHU, Varanasi, India
- Sunday, October 13, 2013
- Sunday, November 03, 2013
- Wednesday, November 20, 2013
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Objective
The objective was to assess the efficacy of intraoperative ultrasound in spinal intradural space occupying lesion.
Methods
We prospectively performed intraoperative ultrasound in 87 patients of spinal intradural space occupying lesion admitted at our university hospital. Intraoperative ultrasound with SonoSite, 180 plus hand carried ultrasound system with c11/7-4 Mhz curved array transducer probe was done in all cases . Extradural tumors, abcess,metastasis have been excluded from this study. A preoperative Magnetic resonance imaging was preformed in all patients. Preoperative and postoperative neurological function was assessed.
Observations
Intraoperative ultrasound examination is excellent in localizing intradural space occupying lesions. Intraoperative ultrasound helps in planning the durotomy. In cases of small spinal tumors especially intramedullary tumors intraoperative ultrasound helps in pinpointing the location of tumor beneath the dura. Laminectomy or laminotomy can be extended if necessary according to size and location identified with repeated peroperative ultrasonic examination. Intraoperative ultrasound helps in delineating the completeness of resection. Residual tumor left if any was excised.
Conclusion
Intraopeative ultrasound is portable, does not require any specialized setup, provides real time images, cost effective, can be repeated as and when required during the procedure with minimum scanning time, and ensures patient and operator safety.
Keywords
Intraoperative ultrasound, intradural tumors, intramedullary tumors, intradural extramedullary space occupying lesions.
Introduction
Spinal cord tumors account for approximately 10% of the central nervous system (CNS) tumors, and one third of them represent primary tumors of the spinal cord. Surgical treatment of spinal cord tumors has been commenced in the beginning of the twentieth century[1]. The intraoperative ultrasound imaging in spinal cord tumor surgery was applied by Reid in 1978[2]. The use of phased-array probes, smaller dimension probes sparked new interest in use of ultrasonography in neurosurgery[4,10].Spinal tumor surgery mainly aims for tumor removal while preventing damage to the surrounding vital neural tissue. This study aims to assess the efficacy of intraoperative ultrasonography (IOUSG) for the surgical management of spinal cord tumors
Patients and Methods
This prospective study included 87 cases of spinal space occupying lesion treated as indoor patient in the Department of Neurosurgery, Institute of Medical Sciences, Banaras Hindu University. The cases registered between the period of 1st August 2011 to 30st September 2013 formed materials for this prospective study. Extradural tumors, abcess and metastasis have been excluded from this study.The mean age of the patients was 41 (+/- 22) years and the male to female ratio was 41 to 46 in spinal cases.The detailed clinical history, including name, age, sex, social status and history related to etiological factors were taken. Age of onset and duration of the disease were also noted. Thorough physical examination was performed. Any local source of infection or scar marks for trauma were noted.The Chief Complaints like limb weakness ,radiating pain,sensory loss, bowel bladder involvement were noted. Past history like previous operation and radiation, time of onset of symptoms, post trauma Intervention, type of intervention, outcome of intervention were noted. Preoperative magnetic resonance imaging was done. Intraoperative ultrasound with SonoSite, 180 plus hand carried ultrasound system with c11/7-4 Mhz curved array transducer probe (Bothell, Washington ,USA) was done in all cases.
Intraoperative Details
Intraoperative ultrasound with SonoSite, 180 plus hand carried ultrasound system with c11/7-4 Mhz curved array transducer probe was done in all cases. The ultrasound probe, covered with an aseptic sheath was placed directly on the surface of the dura mater exposed by laminectomy/laminotomy, and saline was used as the acoustic coupling agent. The probe was manipulated on the examining surface to obtain views of the lesion through the windows formed by the removal of bone. In all the cases, 7-4 MHz transducer was used, with an optimal resolution at a depth range of 0.5- 15 cm, thus enabling the visualization of the structures in the spinal canal. Following the laminectomy or haemilaminectomy, thorough hemostasis was achieved. The surgical cavity was filled with sterile saline and evaluation of the lesion was done by movement of the ultrasound probe over the exposed dura. The process of evaluation with intraoperative ultrasound took approximately 2-4 minutes. A series of 4-5 ,2D ultrasound images were produced. Intraoperative ultrasonographic finding like tumor location, dimension, relationships with the surrounding anatomical structures, solid /cystic, homogeneous/heterogeneous echogenicity, intratumoral cyst/necrosis/hemorrhage and extent of resection at the end of surgery were noted. Patients were closely monitored in an ICU setting to monitor their neurologic examination and acutely detect any neurologic deterioration.
Observations
This prospective study included a total number of 87 patients admitted in the Department of Neurosurgery in our university hospital from 2011 to 2013. Majority of the patients (38, 43.68%) were in the age group of 21-40 year, the average age was 32.5 year. There were 30 patients in the age group of 41-60years, 14 patients in the age group of 0-20 years and 5 patients in the 61 & above years age group with mean age of 49.2, 11.3 and 62 respectively. The younger patient was 9 year old while the oldest was 66 year old. The male patients were outnumbered by the female counterparts (47.13% vs 52.87%). Among intramedullary tumors (n=14) Ependymomas & Astrocytomas were most commonly found in cervical region, where as Hemangioblastoma Epidermoid were found in thoracic region. [Fig 1,2]

Fig.1: Intra-Medullary lesion in upper Dorsal MRI T2 weighted

Fig.2: Intraoperative ultrasound showing the hypoechoic area in the cord of Fig 1 lesion
Among the intradural Extramedullary tumors (n=73), Neurofibroma was most commonly found in cervical region, whereas Meningioma & subpial Lipoma in thoracic region and filum terminale Ependymoma in lumbosacral area.[Table1]
| Intramedullary(n=14) |
|
n |
Cervical |
Thoracic |
Lumbosacral |
| Ependymoma |
04 |
04 |
- |
- |
| Astrocytoma |
05 |
03 |
02 |
- |
| Hemangioblastoma |
01 |
- |
01 |
- |
| Epidermoid |
01 |
- |
02 |
- |
| Metastasis |
02 |
- |
02 |
- |
| Intradural Extramedullary(n=73) |
| Meningioma |
15 |
- |
15 |
- |
| Neurofibroma |
38 |
21 |
11 |
08 |
| Filum terminale Ependymoma |
18 |
- |
08 |
10 |
| Subpial Lipoma |
02 |
- |
02 |
- |
Intramedullary Ependymoma (n=14) was isoechoic in 4 cases [Fig 3,4]
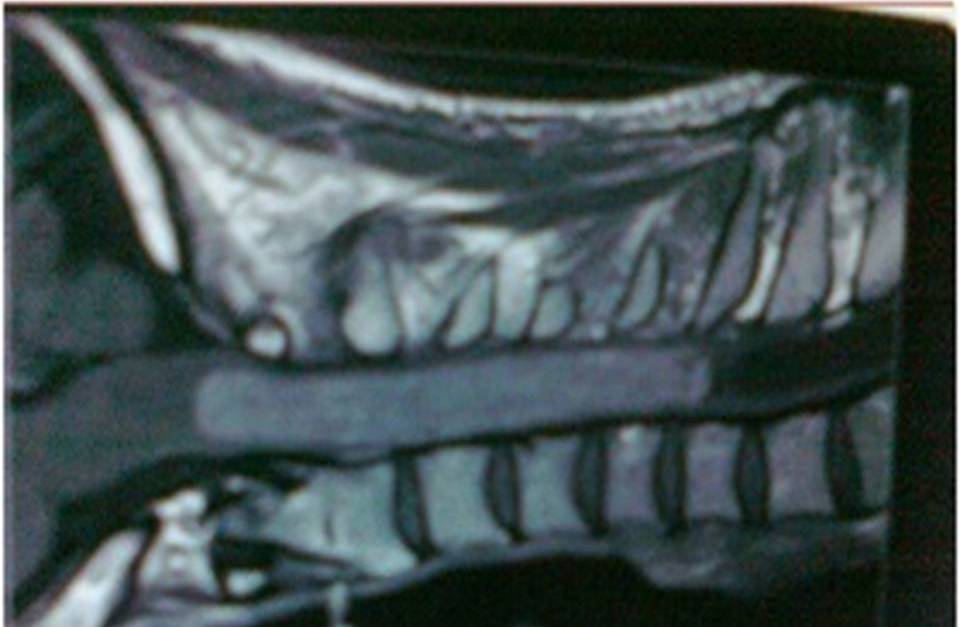
Fig.3: Intramedullary cervical Space occupying lesion in MRI

Fig.4: Intraoperative ultrasound showing hyperechoeic picture inside cord of lesion of Fig 3
and associated with cyst in 4 cases, syrinx in 2 cases and perifocal edema in 3 cases.Astrocytoma was isoechoic in 5 cases and was associated with, syrinx in 3 cases and perifocal edema in 4 cases. Hemangioblastoma, Epidermoid & metastasis were found to be hyperechoic. Among intradural extramedullary tumors (n=73), Meningioma, Neurofibroma, filum terminale Ependymoma Lipoma were hyperechoic. [Fig 5,6]

Fig. 5: Intraspinal anterior cervical lesion in MRI

Fig.6: Lesion seen through intraoperative ultrasound as in Fig 5
Cyst formation was seen in 10 cases of Neurofibroma & 7 cases of filum terminale Ependymoma .[Table 2].
| Intramedullary(n=14) |
|
Hyperechoic |
Isoechoic |
Cyst |
Syrinx |
Perifocaledema |
| Ependymoma |
- |
04 |
4 |
2 |
3 |
| Astrocytoma |
- |
05 |
- |
3 |
4 |
| Hemangioblastoma |
01 |
- |
- |
- |
- |
| Epidermoid |
- |
- |
- |
- |
| Metastasis |
02 |
- |
- |
- |
- |
| tradural Extramedullary(n=73) |
| Meningioma |
15 |
- |
- |
- |
- |
| Neurofibroma |
38 |
- |
10 |
- |
- |
| Filum terminale Ependymoma |
18 |
|
7 |
- |
- |
| Subpial lipoma |
2 |
- |
- |
- |
- |
Discussion
Zhou et al, [2011] evaluated 30 patients with suspected intradural spinal tumors undergone surgery with the aid of IOUS. [1].There were 13 patients with intramedullary tumors (Ependymoma = 2, Astrocytoma = 5, Hemangioblastoma = 2 and metastasis = 4); and 14 patients with extramedullary tumors (Meningioma = 6, Neurinoma = 6, filum terminale Ependymoma = 1 and Lipoma = 1) in their study. They concluded that IOUS is a sensitive intraoperative tool.Toktas et al 2012, evaluated 26 patients with intradural spinal cord tumors surgically treated under intraoperative ultrasonographic guidance. [12].Out of 26 patients, fourteen patients had extramedullary and twelve patients had intramedullary tumors. They found that Intraoperative ultrasonography is practical, reliable and enhances surgical orientation, but also reduces morbidity and helps to resect the tumor completely. The gross tumour excision, partial decompression or a biopsy for tissue diagnosis is usually obtained [13]IOUS may aid the surgeon in visualization of mass and evaluate the extent of removal of mass at surgery [14] .IOUS can identify the level of maximum cord enlargement especially in case of intramedullary tumors before durotomy. A single microsurgical biopsy at the site identified by IOUSG may be enough to establish a tissue diagnosis and damage to the spinal cord tissue and post operative neurological complications can be prevented. The main drawbacks of intraoperative CT is extra radiation exposure during surgery,additional radiologic staff dedicated for intraoperative purposes and the exorbitant cost. The main difficulty with the use of intraoperative MRI are requirement of non-ferromagnetic instruments, MR-compatible devices including operating microscope, additional technician & dedicated neuroradiologist, additional 60 to 90 minutes of anaesthesia. IOUS is a cheaper solution and it is safe for both the patient and operator. Limitations of IOUS are acoustic interference by blood, haemostatic material and air bubbles. Clear echogenic views can only be obtained after sufficient bone element removal to manoeuvre the ultrasound probe. In case of intramedullary tumor surgery IOUS image can be isoechoic further confounding problem in delineating the tumor tissue from normal neural tissue. The high sensitivity ease of use and safety is well in favour of this modality.
Conclusions
IOUS is portable, doesnot require any specialized setup, provides real time images, cost effective, can be repeated as and when required during the procedure with minimum scanning time, and ensures patient and operator safety. IOUS can be performed without increasing operation time significantly; it might even shorten it because it increases the surgeons feeling of safety.
Conflict of Interests
NONE
Authors’ Contribution
NONE
Funding
Nil
Ethical Considerations
NONE
Acknowledgement
NONE
References
[1]Sciubba DM, Liang D, Kothbauer KF, Noggle JC, Jallo GI: The evolution of intramedullary spinal cord tumor surgery. Neurosurgery 2009; 65:84-91.[pubmed].
[2]. Reid MH: Ultrasonic visualization of a cervical cord cystic astrocytoma. AJR Am J Roentgenol 1978; 131:907-908.[pubmed]
[3]Dohrmann GJ, Rubin JM. History of intraoperative ultrasound in neurosurgery. Neurosurg Clin N Am 2001;12:155–66.[pubmed]
[4]Kolstad F, Rygh OM, Selbekk T, Unsgaard G, Nygaard OP. Three-dimensional ultrasonography navigation in spinal cord tumour surgery. Technical note. J Neurosurg Spine 2006;5:264–70.[pubmed]
[5]Miller D, Heinze S, Tirakotai W, Bozinov O, Sürücü O, Benes L, et al. Is the image guidance of ultrasonography beneficial for neurosurgical routine? Surg Neurol 2007;67:579–87.[pubmed].
[6]Sure U, Benes L, Bozinov O, Woydt M, Tirakotai W, Bertalanffy H. Intraoperative landmarking of vascular anatomy by integration of duplex and Doppler ultrasonography in image-guided surgery. Technical note. Surg Neurol 2005;63:133–41.[pubmed]
[7]Tirakotai W, Miller D, Heinze S, Benes L, Bertalanffy H, Sure U. A novel platform for image-guided ultrasound. Neurosurgery 2006;58:710–8.[pubmed]
[8]Van Velthoven V.Intraoperative ultrasound imaging: comparison of pathomorphological findings in US versus CT, MRI and intraoperative findings. ActaNeurochir Suppl 2003;85:95–9.[pubmed]
[9]Woydt M, Krone A, Soerensen N, Roosen K . Ultrasound-guided neuronavigation of deep-seated cavernous haemangiomas: clinical results and navigation techniques. Br J Neurosurg 2001;15:485–95.[pubmed]
[10]Woydt M, Vince GH, Krauss J, Krone A, Soerensen N, Roosen K. New ultrasound techniques and their application in neurosurgical intra-operative sonography. Neurol Res 2001;23:697–705.[pubmed]
[11]Zhou H, Miller D, Schulte D, Benes L, Bozinov O Sure U, Bertalanffy H. Intraoperative ultrasound assistance in treatment of intradural spinal tumours. Clinical Neurology and Neurosurgery 2011;113 :531– 537.[pubmed]
[12]Toktas Z, Sahın S, Koban O, Sorar M, Konya1 D. Is Intraoperative Ultrasound Required in Cervical Spinal Tumors? A Prospective Study. Turk J Neurosurg Received: 02.09.2012 / Accepted: 27.12.2012[pubmed]
[13]Quencer RM, Montalvo BM, Green BA, Eismont FJ.Intraoperative spinal sonography of soft-tissue masses of the spinal cord and spinal canal. AJR Am J Roentgenol 1984; 143: 1307-1315.[pubmed]
[14]Regelsberger J, Langer N, Fritzsche E, Westphal M. Intraoperative ultasound ofintra and extramedullary tumours. Ultraschall Med 2003; 24:399-403 [pubmed]

