
Floor of mouth cysticercosis
1Naveen Sharma,1Vineeta Srivastava,1Vineeta Srivastava “Ravi”,2Mohan Kumar,1Manoj Pandey
- 1Departments of Surgical Oncology Institute of Medical Sciences Banaras Hindu University, Varanasi 221 005 India
- 2Departments of Surgical Pathology Institute of Medical Sciences Banaras Hindu University, Varanasi 221 005 India
- Submitted: June 13, 2012;
- Accepted July 26, 2012
- Published: July 30, 2012
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction:
Isolated cysticercosis of the oral cavity is rare and only a handful of cases has been reported.
Case report:
A 22 year old women presented with a cystic swelling in the floor of mouth. She underwent excision with a diagnosis of mucous cyst and the histology was repoted as cysticercosis.
Discussion:
Mucous retention cyst and minor salivary gland tumors are two common differential diagnosis of cysticercosis
Introduction
Cysticercosis is the larval stage of the tape worm Taenia solium found in tissues whereas the adult worm form is found in the intestines [1]. The eggs, after ingestion of contaminated food, release larvae in the intestine, which penetrate the intestinal wall and migrate to various sites with an affinity for neck, tongue and trunk, subcutaneous tissues and brain [1]. Oral cysticercosis is a rare event, and it represents difficulty in clinical diagnosis [2]. The most frequently involved oral locations are the tongue, labial or buccal mucosa [3,4]. A case of sublingual cysticercosis is being reported.
Case report
A 22 years old female presented with a soft tissue swelling in the floor of mouth. Examination revealed a soft cystic 1.5 cm swelling in the floor of mouth, rest of the oral cavity and the neck was normal. With a clinical diagnosis of a minor salivary gland tumor or a mucus retention cyst, patient underwent wide local excision of the swelling in order to make it the definitive surgery. The histology of the resected specimen showed the swelling to be a cysticercus
(Figure 1). The patient was prescribed Albendazole for 18 months, and is well on follow-up.
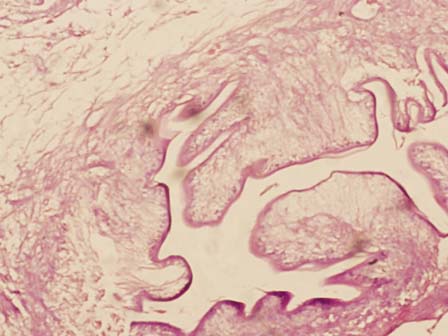
Figure 1: Photomicrograph showing cysticercosis
Discussion
Taenia solium is usually acquired by the ingestion of eggs in the food contaminated with feces. Humans are the only definite host, with pigs serving as intermediate hosts only. The larvae hatch in the small intestinal lumen and penetrate the wall to reach their site of encystations commonly subcutaneous tissue, skeletal muscle, brain and head and neck region. The cysticerci in the brain are the most serious manifestation and may be life threatening. CNS lesions are diagnosed by imaging while other accessible lesions are usually diagnosed by excision and histology. Cysticercosis of the oral cavity is rare only a handful of cases have been reported earlier [5-9]. Floor of mouth lesions are rarest among all oral lesions. Oral lesions may appear as mucocoel and may be diagnosed as minor salivary tumors [10], which is the most common differential clinical diagnosis. These patients have to receive medical therapy in the form of Albendazole or Praziquantel, with Niclosamide sometimes being added for CNS lesions. The patient described here underwent surgery as the definitive and diagnostic procedure and is doing well on anti helminthic agents.
Authors' Contribution
NS: Did the literature search and prepared the draft manuscript
VS: Did the literature search and helped in preparation of manuscript
DKR: Preparation of draft manuscript
MK: Helped with the pathological part of manuscript
MP: concept and design, review and revision of manuscript.
Conflict of Interests
The authors declare that there are no conflicts of interest
Ethical Considerations
Written consent was obtained from the patient for publication of this case report
Funding
None
References
[1]. Jay A, Dhanda J, Chiodini PL, Woodrow CJ, Farthing PM, Evans J, Jager HR. Oral cysticercosis. Br J Oral Maxillofac Surg. 2007; 45(4): 331-4. Epub 2006 Jan 18. [Pubmed]
[2]. Sathe NU, Acharya RG, Patil M, Bhatia A, Chiplunkar D. An unusual case of labial cysticercosis with a natural history. Natl J Maxillofac Surg. 2011; 2(1): 100-2.[Pubmed]
[3]. Singh S, Chhabra S, Aggarwal G, Kalra R, Duhan A, Sen R. Oral cysticercosis-a rare presentation. Asian Pac J Trop Med. 2011; 4(7): 587-8.[Pubmed]
[4]. Delgado-Azañero WA, Mosqueda-Taylor A, Carlos-Bregni R, Del Muro-Delgado R, Díaz-Franco MA, Contreras-Vidaurre E. Oral cysticercosis: a collaborative study of 16 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 103(4): 528-33. Epub 2006 Aug 2.[Pubmed]
[5]. de Souza PE, Barreto DC, Fonseca LM, de Paula AM, Silva EC, Gomez RS. Cysticercosis of the oral cavity: report of seven cases. Oral Dis. 2000; 6(4): 253-5.[Pubmed]
[6]. Timoşca G, Gavriliţă L. Cysticercosis of the maxillofacial region. A clinicopathologic study of five cases. Oral Surg Oral Med Oral Pathol. 1974; 37(3): 390-400.[Pubmed]
[7]. Aggarwal S, Wadhwa N. Swelling on the tongue: a rare presentation of oral cysticercosis. Diagn Cytopathol. 2009; 37(3):236-7.[Pubmed]
[8]. Bhandary S, Singh R, Karki P, Sinha AK. Cysticercosis of tongue--diagnostic dilemma. Pac Health Dialog. 2004; 11(1):87-8.[Pubmed]
[9]. Ribeiro AC, Luvizotto MC, Soubhia AM, de Castro AL. Oral cysticercosis: case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 104(4): e56-8. Epub 2007 Aug 13.[Pubmed]
[10]. Lee KH, Cepeda L, Miller M, Siegel DM. Mucoceles not - Oral cysticercosis and minor salivary gland adenocarcinoma: two case reports. Dermatol Online J. 2009 Jul 15;15(7):8.[Pubmed]

