Case Report

Leiomyoma Jejunum of Small Intestine as Rare Cause of Intestinal Obstruction: Case Report and Review of Literature
1Ana Maria Minaya Bravo, 1Fernando Mendoza Moreno, 1Fernando Noguerales Fraguas, 2Jose Ignacio Busteros, 1 Francisco Javier Granell Vicent
- 1General Surgeon, Príncipe de Asturias Hospital, Alcala de Henares, Madrid. Spain.
- 2Department of Pathology, Príncipe de Asturias Hospital, Alcala de Henares, Madrid. Spain.
- Submitted Saturday, January 25, 2014
- Accepted:Saturday, February 08, 2014
- Published Friday, September 05, 2014
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Leiomyomas are uncommon tumors originated from either circular or longitudinal muscular layer, or muscularis mucosae. They occupy the fourth place of all small intestinal tumors, being the most common benign tumors of the small intestine. The jejunum is the most frequent location, followed by ileum and duodenum. They are the most frequent of all small intestinal tumors producing symptoms. Diagnosis is performed by CT, endoscopy or barium swallow. The behavior of these tumors is defined by the number of mitosis and clinical behavior. Leiomyomas must be treated with surgery. Wide resection is required in order to avoid recurrence. We report a case of leiomyoma which presented as intestinal obstruction, requiring urgent surgery. Leiomyoma is an extremely rare cause of intestinal obstruction and few cases have been described with this presentation in the English literature.
Key Words
Leiomyoma, intestine, obstruction, tumor.
Introduction
Benign small intestinal neoplams account for 1-6% of all gastrointestinal neoplasms. Leiomyomas constitute 20-30% of all benign gastrointestinal tumors [1 2 3]. They are the most common of all small intestinal tumors producing symptoms, and the most frequent benign tumor in the small intestine [1 4].
The peak incidence is in the sixth decade of life and both sexes are affected equally [1 2]. They can be found as an incidental finding in autopsies. However, in other occasions symptoms appear and they range from bleeding to abdominal pain to acute abdominal condition such as obstruction
[1 2 5]. They must be treated with surgery and a wide resection is mandatory [1 2]. We report a case of leiomyoma arising in jejunum which caused an acute intestinal obstruction and requiring urgent surgery, which is an uncommon way of presentation.
Case Report
A 64 year old male with a history of high blood pressure and cholecystectomy was admitted to our Department with abdominal pain, vomiting and inability to pass the flatus and stool for the two last days. The patient was apyrexial and hemodynamically stable. On examination, abdominal distention and periumbilical tenderness were evident. Hematology and biochemistry was normal. Plain abdominal X-ray illustrated dilated jejunum and the rest of small intestine and bowel collapsed. He was diagnosed with intestinal obstruction due to adhesions.
Initially, he was treated with intravenous fluid therapy and bowel rest. After 48 hours, there was clinically worsening and plain abdominal X ray showed a clear worsening (Figure 1) CT scan was performed and it showed a remarkable dilatation of small intestine and sudden change in caliber in the jejunum (Figure 2). Finally, he underwent emergency surgery. A small tumor of 1.5 cm of diameter was found in the terminal jejunum as the cause of acute obstruction. Wide resection with anastomoses was carried out and the patient was discharged after 7 days.

Figure 1: plain abdominal X-ray illustrated an intestinal obstruction

Figure 2: CT illustrates stricture in jejunum and signs of intestinal obstruction
Frozen section biopsy showed 1.5 cm diameter (Figure 3) leiomyoma, number of mitosis less than 1 per HPF and 12 lymph nodes with no tumor. Immunohistochemistry revealed: HHF-35, desmin and smooth muscle actine positive; on the other hand, Ki67 less than 5% and CD 34 and C-kit negative (Figure 4).

Figure 3: Macroscopic examination. A well circumscribed lesion with whitish colour on the cut surface at the submucosae and muscular layer.
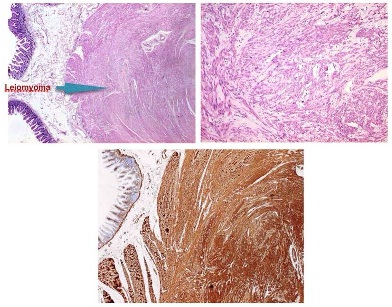
Figure 4: Microscopic examination. Bundles of smooth muscular cells , placed in fascicles and with fusiform appearance without atypia. Inmunohistochemistry revealed muscle -specific actin positive cells.
Discussion
Leiomyoma occupies the fourth place of all small intestinal tumors after lymphoma, adenocarcinoma and leiomyosarcoma [1 4]. According to Good (1963), and Bruneton (1981), jejunum is the most frequent location of leiomyoma, followed by ileum and duodenum [1 2 3]. Leiomyomas have also been reported in appendix and Meckel diverticulum [7 8]. They remain silent for many years, and when symptoms appear they are varied: bleeding (59-70%), abdominal pain (66%) and acute intestinal obstruction (8-13%) [1 3 5]. Palpable mass has also been documented, especially in case of leiomyosarcoma. Some authors have associated leiomyoma to intestinal atresia [1 2 6].
Diagnosis is performed by medical history, physical exam, barium swallow, CT, endoscopy, angiography and capsule endoscopy. CT is a useful tool. Leiomyomas are displayed as ovoid or spheric masses of homogeneous density and provide contrast enhancement. This is an excellent method for distinguishing between leiomyosarcoma and leiomyoma. Leiomyoma, and not leiomyosarcoma, must be considered if size does not exceed 6 cm of size across and no metastases are proven. However, the definitive diagnosis will be carried out with an adequate histopathological study [1 3 5].
According to Skandalakis and Gray (1964), leiomyomatosis neoplasms of small intestine are originated in either the circular or longitudinal muscular layer, or muscularis mucosae [3 6].
It is important an adequate inmunohisyopathological study in order to differentiate leiomyoma from GIST. Leiomyomas show positive stain for actin and deeming and negative CD 34 and CD 117. However, GISTs present positive CD34 and CD117. Leiomyomas can be classified into three groups: benign, malignant and, between both of them, a third category called leiomyoblastoma which is not considered a malignant neoplasm. Albeit lymph nodes and hepatic metastases have been reported in some of the cases [3]. Malignancy is determined by the number of mitoses. If it exceeds 10 per high per field, malignancy is an assumption. On the other hand, the clinical behavior also influence
The diagnosis of benign nature is made by number of mitosis below 10, and a 2 year free disease period [1 2 3]. Four patterns of growth have been described: intraluminal, intramural, extraluminal and dumbbell shaped [1]. In the small intestine, the most frequent type is extraluminal followed by intraluminal. We report a case of intramural growth.
Treatment is surgery to avoid the risk of malignancy in the future. Wide resection is mandatory due to the tendency to recur locally even after many years [1 2]. Prognosis of leiomyomas after surgery is excellent [2].
Conclusions
Leiomyomas are infrequent tumors and few cases have been reported in the English literature. We report an interesting case of leiomyoma which presented as intestinal obstruction and required an urgent surgery. The case highlights that small leiomyomas can originate intestinal obstruction and appear as an acute abdominal condition. So, these tumors must be considered in the differential diagnosis of intestinal obstruction.
Learning Points
Leiomyoma of jejunum is a rare cause of intestinal obstruction which requires urgent surgery.
Leiomyoma occupies the fourth place among all small intestinal tumors.
CT is a helpful tool. However, the definitive diagnosis is made with an adequate histopathological study.
The term benignancy is defined by absence of mitosis and a 2 year free disease period. Treatment is surgery with wide resection in order to avoid recurrence locally
Author Contributions
AMMB: designed the paper, drafted and revised it .
FMM: collected data and Pubmed
.
FNF: revised the paper
JIB: histopathological contribution.
FJGV: revised the paper.
Conflict of Interests
The authors declare that there are no conflicts of interests.
Ethical Consideration
The written informed consent was obtained from the patient for publication of this case report.
Funding
None declared
Acknowledgement
None
References
[1].Sunamak O, Karabikak I, Aydemir I, Aydogan F, Guler E, Cetinkaya S, et al. An intraluminal leiomyoma of the small intestine causing invagination and obstruction: a case report. Mt Sinai J Med 2006;73(8):1079-81[Pubmed]
[2].Wilson SL, Wheeler ME. Giant leiomyoma of the small intestine with free perforation into the peritoneal cavity. South Med J 1992;85(6):667-8 [Pubmed]
[3].Gourtsoyiannis NC, Bays D, Malamas M, Barouxis G, Liasis N. Radiological Appearances of the small intestinal leiomyomas. Clin Radiol 1992;45(2):94-103 [Pubmed]
[4].Tervit GJ, Forster AL. Leiomyoma of the small intestine in an 11 year old boy. Eur J Pediatr Surg 1997; 7(1):44.[Pubmed]
[5].Goren G, Zelikowski A, Abu-Dalu J, Urca I. Leiomyoma of the jejunum as the cause o fan acute abdominal condition: report of a case. Dis Colon Rectum 1974;17(6):782-5.[Pubmed]
[6].Ince E, Oğuzkurt P, Canpolat ET, Temiz A, Hiçsönmez associated with ileal atresia: a case report. J Pediatr Med 2013;48(3):33-5.A. Congenital leiomyoma of the distal ileum [Pubmed]
[7].Hertzog MS, Chacko AK, Pitts CM. Leiomyoma of terminal ileum producing a false-positive Meckel´s scan. J Nucl Med 1985;26(11):1278-82.[Pubmed]

