Case Report

A Rare Complication after Laparoscopic Appendectomy: Septic Thrombosis of Superior Mesenteric Vein
1Erdal Uysal, 2Mehmet Alı Ikidag 3Mehmet Dokur,4Basar Aksoy
- 1Department of General Surgery-and Transplantation Center, Sanko University Hospital, Gaziantep, Turkey
- 2Department of Radiology, Sanko University Hospital Gaziantep,Turkey
- 3Department of Emergency, Gaziantep, Turkey,
- 4Department of General Surgery, Sanko University Hospital, Gaziantep, Turkey.
- Submitted: Saturday, December 20, 2014
- Accepted: Sunday, January 18, 2015
- Published: Monday, February 02, 2015
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Introduction
Septic pylephlebitis and thrombosis of superior mesenteric vein is a rare but life threatening complication of acute appendicitis. The aim of this presentation is to share our experience in diagnosis and management of a patient with septic thrombosis of superior mesenteric vein (SMV) encountered after laparoscopic appendectomy and to call attention to this rare but fatal entity.
Case Presentation
A 28 years old male presented to the emergency room with complaints of fever and severe abdominal pain. He had a history of laparoscopic appendectomy 1 week ago in another hospital. His body temperature was 39.5 degree C, White Blood Cell was 10.7 103/mm3, C Reactive Protein was 118 mg/dl. The patient underwent contrast enhanced computed abdominal tomography examination for etiological work up. There were endoluminalthrombus and increase in the diameter of superior mesenteric vein in its 8 centimeters segment. The patient was hospitalized, parenteral systemic antibiotic therapy was started with third generation cephalosporin and metronidazole. Also anticoagulant medication was started, with subcutaneous low molecular weighted heparin, 1mg/kg, and twice a day. Control computed abdominal tomography performed 1 week later showed partial decline in the size of thrombus and diameter of superior mesenteric vein. Heparin was switched to warfarin, and the patient was discharged. In his third week control, he was symptom free and laboratory findings were in normal ranges.
Conclusion
Septic pylephlebitis and thrombosis of superior mesenteric vein is a rare but life threatening complication of acute appendicitis. Parenteral anticoagulants and antibiotics are the first choice in the treatment and should be started immediately; interventional radiology or surgical treatment may be used in selected cases. Contrast enhanced computed abdominal tomography is the first choice among radiological modalities in diagnosis.
Key words
appendectomy, septic thrombosis, superior mesenteric vein
Introduction
Septic pylephlebitis and thrombosis of superior mesenteric vein is a rare but life threatening complication of acute appendicitis. It is usually caused secondary to infections of organs that have venous drainage to portal system [1]. It is often seen in septic conditions as diverticulitis or cholangitis. Sometimes thrombus is seen in portal vein, superior or inferior mesenteric veins. It is usually not considered in the differential diagnosis of post appendectomy abdominal pain, as it is rare and does not have any specific signs or symptoms, and delay in the diagnosis may occur, which may lead to late management and increase in mortality [2].
The aim of this presentation is to share our experience in diagnosis and management of a patient with septic thrombosis of superior mesenteric vein (SMV) encountered after laparoscopic appendectomy and to call attention to this rare but fatal entity.
Case Report
A 28 years old male presented to the emergency room with complaints of fever and severe abdominal pain. He had a history of laparoscopic appendectomy 1 week ago in another hospital. He had widespread tendency on palpation, prominently in epigastric region. There was no abdominal defense or rebound. His body temperature was 39.5 0C, blood pressure was 120/80 mmHg, pulse 112/min, respiration rate was 25/min. Blood test results were as follows: White Blood Cell 10.7 103/mm3(4,8-10.8 mm3), aspartate transaminase 34 U/L (5-34 U/L), alanine transaminase 62 U/L (0-55U/L ), Amylase 59, total bilirubin 1 mg/dl and C Reactive Protein (CRP) 118 mg/dl (0.0-5.0 mg/dl ).
The patient underwent contrast enhanced abdominal computed tomography (CT) examination for etiological work up. There were endoluminalthrombus and increase in the diameter of superior mesenteric vein (SMV) in its 8 centimeters segment (Figure 1,2). The patient was hospitalized; parenteral systemic antibiotic therapy was started with third generation cephalosporin and metronidazole. Also anticoagulant medication was started, with subcutaneous low molecular weighted heparin, 1mg/kg, and twice a day. Oral intake was stopped, parenteral nutrition with intravenous fluid and electrolytes were given.
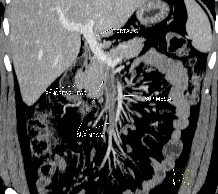
Figure 1-Coronal MIP contrast enhanced CT images on venous phase show increased diameter of superior mesenteric vein endoluminalthrombus reaching to the portal venous confluence
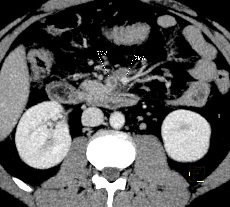
Figure 2-Axial MIP contrast enhanced CT images on venous phase show increased diameter of superior mesenteric vein endoluminalthrombus reaching to the portal venous confluence
In the second day of hospitalization, there was relief in his symptoms and laboratory findings improved. Oral intake was started on third day. Control abdominal CT performed 2 week later showed partial decline in the size of thrombus and diameter of SMV (Figure 3). No bacteria were isolated in the blood culture. Heparin was switched to warfarin, and the patient was discharged. In his third week control, he was symptom free and laboratory findings were in normal ranges.

Figure 3-Axial MIP contrast enhanced CT image on venous phase after treatment shows decreased caliber of Superior mesenteric vein with respect to prior images and luminal contrast enhancement suggesting recanalization
Discussion
Septic pylephlebitis and thrombosis of superior mesenteric vein is a rare but life threatening complication of acute appendicitis. It is usually caused secondary to infections of organs that have venous drainage to portal system [1]. It is often seen in septic conditions as diverticulitis or cholangitis. Although the incidence is ever-decreasing due to advances in surgery methods and use of wide spectrum new generation antibiotics, it still has high mortality as 30-50% [3 4]. It may have various clinical signs and symptoms, but patients usually refer with nonspecific complaints like abdominal pain and fever. There is no specific laboratory clue, white blood cell counting and CRP levels may be increased. Escherichia coli, bacteroides, Klebsiella and enterobacters may grow in blood cultures. Our case was also admitted with nonspecific symptoms, fever and abdominal pain with widespread tendency on palpation, prominently in epigastric region. There was no abdominal defense or rebound. There was no bacteria growth in the blood culture, despite fever and increased CRP [5 6].
Computed abdominal tomography is the first choice among radiological modalities to show mesenteric vessels and exclude other differential diagnosis such as intra-abdominal abscess [7 8].
Anticoagulant medication must be started as soon as possible to prevent septic complications and to maintain venous circulation. Interventional radiology or surgical treatment may be used in selected cases [1,9], however, parenteral anticoagulants and antibiotics are the first choice in the treatment [4 10 11]. Surgical thrombectomy has been successfully used via iliocolic vein in a previous study [1]. We did not perform any surgical procedure to our patient since he responded rapidly to the medical treatment. In the first 10 days, low molecular weighted heparin was given, then switched to warfarin.
In cases with insufficient or negative response to medication and continuing of abdominal pain, peritonitis or intestinal necrosis should be suspected and laparotomy must be performed. Patients must be investigated about predisposing conditions such as protein-S deficiency or factor-VII abnormalities [12], so we referred the patient to the hematology department.
Conclusion
Septic pylephlebitis and thrombosis of superior mesenteric vein is a rare but life threatening complication of acute appendicitis. Parenteral anticoagulants and antibiotics are the first choice in the treatment and should be started immediately, interventional radiology or surgical treatment may be used in selected cases. Abdominal CT is the first choice among radiological modalities in diagnosis.
Learning points
Septic pylephlebitis and thrombosis of superior mesenteric vein is a rare but life threatening complication of acute appendicitis. Parenteral anticoagulants and antibiotics are the first choice in the treatment.
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available
with authors.
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
EU helped in acquisition of data and preparation of the first draft, EU, MD and MAI was responsible for conception of the idea, overall preparation and revision of the manuscript, EU and MAI and BA was responsible for management of the patient and revising the manuscript for important intellectual content. All authors read and approved the final manuscript
References
[1].Nishimori H, Ezoe E, Ura H, Imaizumi H, Meguro M, Furuhata T, Katsuramaki T, Hata F, Yasoshima T, Hirata K, Asai Y. Septic thrombophlebitis of the portal and superior mesenteric veins as a complication of appendicitis: report of a case. Surg Today. 2004;34:173-6[Pubmed]
[2].Chang YS, Min SY, Joo SH, Lee SH. Septic thrombophlebitis of the porto-mesenteric veins as a complication of acute appendicitis.World J Gastroenterol. 2008 Jul 28;14:4580-2 [Pubmed]
[3]Plemmons RM, Dooley DP, Longfield RN. Septic thrombophlebitis of the portal vein (pylephlebitis): diagnosis and management in the modern era. ClinInfect Dis. 1995; 21: 1114–1120.[Pubmed]
[4].Chang PK, Hsu KF, Yu JC, Chang YM, Chan DC, Liao GS Acute appendicitis with superior mesenteric vein septic thrombophlebitis. JSLS. 2006;10:108-13 [Pubmed]
[5].Lim HE, Cheong HJ, Woo HJ, Kim WJ, Kim MJ, Lee CH, Park SC. Pylephlebitis associated with appendicitis. Korean J Intern Med. 1999;14:73-6 [Pubmed]
[6].Plemmons RM, Dooley DP, Longfield RN. Septic thrombophlebitis of the portal vein (pylephlebitis): diagnosis and management in the modern era. Clin Infect Dis. 1995;21:1114-20. [Pubmed]
[7].Balthazar EJ, Gollapudi P. Septic thrombophlebitis of the mesenteric and portal veins: CT imaging.JComput Assist Tomogr. 2000;24:755-60 [Pubmed]
[8].Saxena R, Adolph M, Ziegler JR, et al. Pylephlebitis: A case report and review of outcome in the antibiotic era. Am J Gastroenterol. 1996;91:1251–3 [Pubmed]
[9].Wichman HJ, Cwikiel W, Keussen I.Interventional treatment of mesenteric venous occlusion. Pol J Radiol. 2014:30;79:233-8 [Pubmed]
[10].Stitzenberg KB, Piehl MD, Monahan PE, Phillips JD. Interval laparoscopic appendectomy for appendicitis complicated by pylephlebitis.JSLS. 2006;10:108-13. [Pubmed]
[11].Condat B, Pessione F, Helene Denninger M, Hillaire S, Valla D. Recent portal or mesenteric venous thrombosis: increased recognition and frequent recanalization on anticoagulant therapy. Hepatology. 2000;32:466-70 [Pubmed]
[12].Chen MC, Brown MC, Willson RA, Nicholls S, Surawicz CM. Mesenteric vein thrombosis. Four cases and review of the literature. Dig Dis. 1996;14:382-9.[ [Pubmed]M

