Case Report

Adult Intussusception- A Rare Diagnostic and Therapeutic Dilemma
Ravi Shankar J C
Department of General Surgery, Karnataka Institute of Medical Sciences, Hubli, Karnataka, India-580022
This is an Open Access article distributed under the terms of the
Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background
Intussusception is one of the most common causes of acute abdominal pain. The majority of cases are idiopathic and ileocolic in location. This entity is highly common in paediatric age group than the adults. Colocolic intussusception is an uncommon type of intussusception that is usually associated with a pathologic lead point.
Case presentation
A 57 year-old male patient presented with the complaint of dull aching pain in his right lower abdomen since 1 month. Investigations revealed a submucous lesion near hepatic flexure. Intra operatively colo-colic intussusception was noted with a submucosal lipoma.
Conclusions
Uncommon age group, where malignancies are common and also the uncommon type, makes this entity a difficult situation to manage. Here, we tried to highlight some aspects which are important for its management.
Keywords
Adults; Colo-colic; Intussusception; Lipoma; Pain abdomen.
Introduction
Abdomen is known as “the magic box”. A common condition may present in an uncommon age group or an uncommon presentation may bring light to the underlying pathology. Such surprises widen our aura and awe towards medicine. Here is one such report of rare presentation of intussusception.
Intussusception is defined as the invagination of one portion of bowel into an immediately adjacent portion. It is a common cause of acute abdominal pain in children. Rather uncommon in adults, if it occurs, points towards an underlying pathology. Usually it will be an ileo-colic intussusception. This report is a case of intussusception in a 57 year old, a colo-colocolic type. The diagnostic dilemma in such a case lies from the fact that malignancies are to be thought of first than a benign pathology in this age group. The surgical dilemma is to go for a limited resection or radical resection. A light into these dilemmas are sought here.
Case Presentation
A 57 year-old male patient presented with the complaint of dull aching pain in his right lower abdomen since 1 month. On examination, tenderness was elicited in right hypochondrium and lumbar region without any palpable mass and there was a slight increase in bowel sounds. On digital rectal examination, formed stools were present.
Erect X-ray and ultrasonography of the abdomen were normal. Colonoscopy revealed a submucous lesion near hepatic flexure. CT scan demonstrated telescoping of caecum and distal ascending colon into the proximal ascending colon and hepatic flexure respectively (Figure 1a), with a large hypodense lesion measuring 3.5x3.2 centimetres in the hepatic flexure and transverse colon (Figure 1b), CEA and AFP were normal.
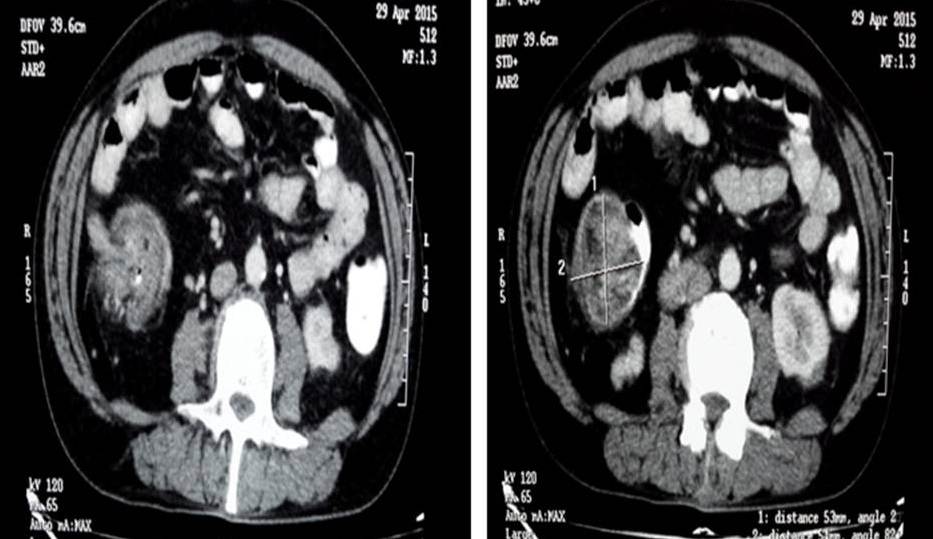
Figure 1: Computed tomography (A) showing sausage shaped
mass suggestive of intussusception (B) showing a non-pedunculated hypodense
lesion near hepatic flexure and transverse colon
Patient was taken up for exploratory laparotomy. Intra operatively colo-colic intussusception was noted with a submucosal lipoma measuring 6x4 centimetres near hepatic flexure (Figure 2a). Resection of involved ascending colon, hepatic flexure and part of transverse colon was performed (Figure 2b), followed by end-to-end anastomosis. Postoperative recovery was uneventful. Histopathological reports were suggestive of lipoma. Patient is in regular follow-up and is symptom-free.
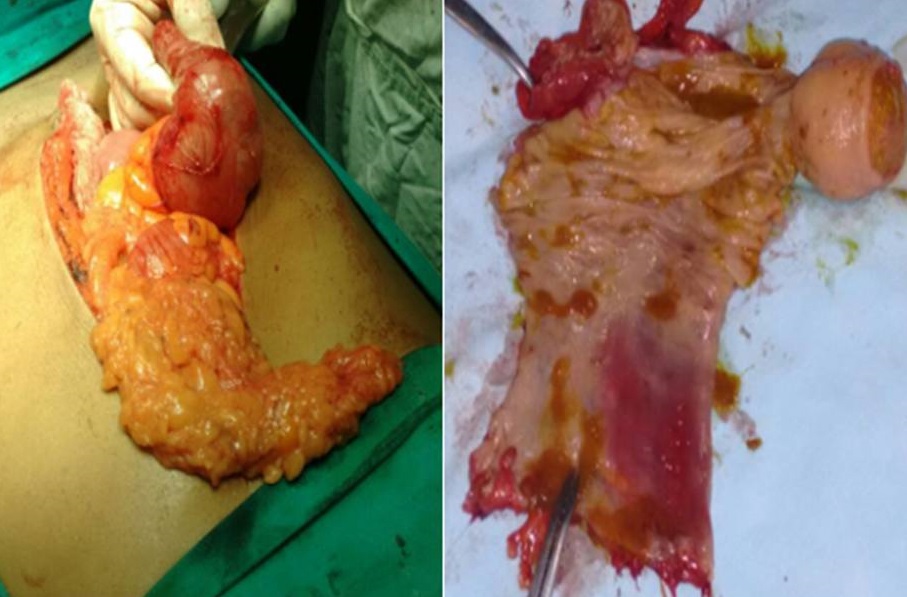
Figure 2: (A) operative picture demonstrating submucosal lesion near hepatic flexure (B) the specimen cut open showing submucosal lipoma with yellowish fatty tissue within the tissue.
Discussion
Adult intussusceptions represent only about 5% of all intussusceptions [1]. The mean age is 54.4 years, and male-to-female ratio is 1:1.3 [2]. Usually asymptomatic, those with symptoms report abdominal cramps, pain, nausea, vomiting and occasionally per rectal bleeding. There may be symptoms of bowel obstruction, especially where the underlying cause is malignant. A palpable abdominal mass is infrequent [3]. Due to vague symptoms and signs of adult intussusception, its preoperative diagnosis is difficult.
There are four types of intussuseption depending on the location namely, ileo-colic, ileo-ileo-colic, colo-colic and small bowel intussusception. The primary mechanism by which intussusception occurs is when an intraluminal mass is pulled forward by peristalsis and drags the attached bowel wall segment with it. Pedunculated tumours, such as adenomatous polyps or lipomas, are the classic examples [4].
Gastrointestinal lipomas are a group of benign tumours which result from proliferations of mature fatty tissue that usually arise in the submucosa and commonly seen in large intestine more on the right side. They make up 0.035-4.4% of all intestinal neoplasms. The majority of symptomatic lesions occur in adults during sixth decade. Lipoma of the colon mimicking adenocarcinoma is rare but poses a difficult clinical dilemma. It can be difficult to separate the two and even endoscopic ultrasound can be nondiagnostic and adequate histology sampling may require a resection [5].
Plain abdominal X-ray findings in intussusception show non-specific results suggestive of bowel obstruction or an ‘air crescent sign’ between the walls of intussusceptum and intussuscipiens [2]. The classic appearance on a sonographic image is called the “doughnut sign” or “target lesion” and represents several concentric rings of bowel. But plain abdominal x-rays and ultrasound are of limited diagnostic value in adults [1]. Abdominal CT is the most useful diagnostic tool not only for detecting an intussusception with a diagnostic yield of 78%, but also to identify the underlying cause. CT appearance is often a complex sausage-shaped soft tissue mass with an eccentric area of fat density contained within, which represents the mesenteric fat [4]. Gastrointestinal lipomas may appear as a smooth, well-circumscribed abdominal mass of fat density (−50 to −100 Hounsfield units) within the lumen of bowel [2].
Treatment is almost always surgical in adults when compared to children. Sometimes submucosal lipoma of the large intestine may masquerade colonic malignancy [5]. In such cases en bloc resection of the lesion using standard oncologic surgical principles is recommended. If intra-operative features are suggestive of a benign pathology, a limited resection is favoured.
Conclusions
Intussusception in elderly age group is an uncommon occurrence and may present with vague symptoms. Colo-colic intussusception can occur secondary to gastro-intestinal lipomas. CT abdomen is an useful investigation to diagnose such lesions. Sometimes these lipomas may masquerade malignancy and pre-operative differentiation may not be always possible. In such cases, diagnosis can be confirmed intra-operatively, and limited resection is preferred for a benign lesion.
Learning points
Benign conditions like submucosal lipomas in colon can rarely occur in elderly age group.
They mimic malignancy and should be carefully investigated to confirm the diagnosis.
Limited resection is the treatment for such benign lesions.
Authors’ contribution
RS carried out the literature search prepared and edited the manuscript.
Ethical Consideration
Written informed consent was obtained from the patient for publication of this Case Report and any accompanying images.
Competing Interests
The authors declare that they have no competing interests
References
1.Soni S, Moss P, Jaiganesh T. Idiopathic adult intussusception. International Journal of Emergency Medicine 2011 4:8. doi:10.1186/1865-1380-4-8.
[Pubmed]
[PMC
full text]
2.Wani I, Muzafar I. Ileo-ileal intussusception in an adult by lipoma, OA Case Reports 2013 May 01;2(4):32. [Full text]
3.Dungerwalla M, Loh S, Smart P. Adult colonic intussusception: Surgery still the best option. Journal of Surgical Case Reports 2012 6:3.
[Pubmed]
[PMC
Full text]
4.Bousseaden A, Afifi R, Essamri W, Benelbarahdadi I, Ajana FZ, Benazzouz M,
Essaid A: Adult colocolic intussusception diagnosed by ultrasonography. Journal of Medical Case Reports 2011 5:294.
[Pubmed]
[PMC
Full text]
5.PE Coyne, T Teemul, B Dent, D Henderson, R Crabbe, T Garud. Submucosal lipoma of the large intestine masquerading as a colonic malignancy. J Surg Case Rep 2011, Issue 2, February 2011, Pp 4-4, doi.org/10.1093/jscr/2011.2.4
[Full
text]

