Case Report

Maxillary Ameloblastoma – Management in an oncology centre.
Elizabeth M Iype1, Sajith M Babu1, Pradeep1, Gigi Thomas2
- 1Departments of Surgical Oncology RCC, Trivandrum, India
- 2Departments of community Oncology RCC, Trivandrum, India
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
A case of maxillary ameloblastoma and its management is presented. This case report is being presented to stress the importance of distinguishing maxillary ameloblastoma from malignancy and its treatment by radical resection . Hence it is best managed in an oncology centre where the expertise in surgery, imageology and pathology are present.
Key-words:
odontogenic tumours, ameloblastoma, maxilla
Introduction
Ameloblastoma is a benign tumour arising from the odontogenic epithelium and accounts for 11% of all odontogenic tumours. They are the commonest odontogenic neoplasm affecting the jaws. Approximately 80% of ameloblastomas occur in the mandible, usually in the molar-ramus area. Maxillary ameloblastomas constitute only 20% and are found frequently in the molar area, antrum and floor of the nose [1]. Although the tumour is slow growing, ameloblastoma is unique because of its locally aggressive behavior and a high recurrence rate.
Case report
A 50 year old man was referred to our centre on June 2008 with symptoms of nasal blockade and headache of one year duration. Clinical examination showed no abnormality in facial contour, oral cavity or in dental alignment. On further evaluation by CT scan an isodense mass lesion was found involving the whole of the left maxilla with thinning and expansion of the maxillary bone and with extension in the nasal cavity , ethmoids and infratemporal fossa (Fig.1). A punch biopsy was taken endoscopically from the nasal mass. Histopathological examination showed anastomosing strands, basaloid cells around cystic spaces. The cystic spaces showed pale eosinophilic material laden with hemosiderin which supported the diagnosis of plexiform type of ameloblastoma (Fig.2).
Surgical excision was planned and a subtotal maxillectomy was done due to the extent of the disease. The tumour was seen extending and eroding the posterior and the medial wall of the maxilla with thinning of the anterolateral wall. The tumour was excised with a wide margin preserving only the floor of the orbit . The defect was closed with split thickness skin graft and an immediate obturator was placed over the graft. The final histopathology was consistent with the plexiform type of ameloblastoma and hence no adjuvant treatment was planned . He was subsequently fitted with a permanent obturator for restoring his swallowing and speech. After three years of follow up, the patient is disease free with a good quality of life .
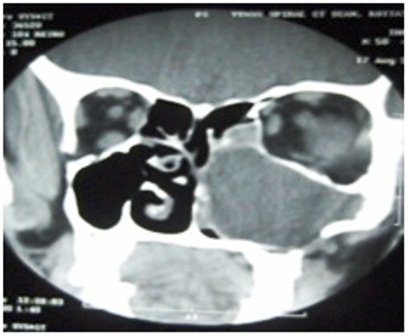
Fig.1 CT scan shows soft tissue density lesion with well defined margins in left maxilla with extension into nasal cavity
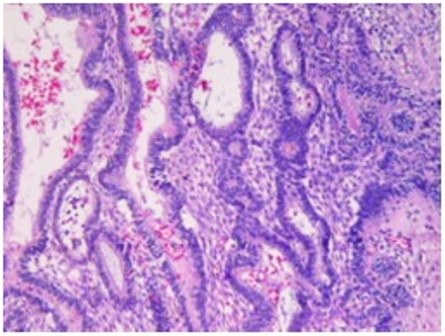
Fig2: H & E X 200.
Columnar cells in a pallisading manner with the nuclei displaced away from the basement membrane and vacuolated cytoplasm in a myxoid stroma. The cystic spaces showed pale eosinophilic material with foamy hemosiderian which supports plexiform type of ameloblastoma
Discussion
Ameloblastoma usually present as slowly enlarging facial swelling or sometimes with pain, loose tooth, and malocclusion. It occurs in all age group, but most commonly in third and fourth decades. The differential diagnosis includes peripheral giant cell granuloma, peripheral ossifying fibroma, odontogenic keratocyst, dentigerous cyst, odontogenic myxoma and ossifying fibroma. Radiologically these tumours are seen as unilocular or multilocular radiolucency . It can thin down the bone and may have scalloped borders with a smooth contour. Computed tomography study is required to aid the diagnosis and to delineate the extent of the tumours in maxilla. Magnetic resonance imaging shows intermediate signal intensity on T1WI and high intensity on T2WI [2]. The histopathological types of ameloblastomas are follicular, plexiform, granular, desmoplastic, basal cell and papillary. Most commonly seen are the plexiform and the follicular types. Histopathologically these tumours contain strands, nests or islands of epithelial cells in a fibrous stroma. [3], [4].
The clinical behavior mimics a low grade malignant tumour due to the aggressive and sometimes infiltrative nature of these tumours. Only few cases of malignant ameloblastic carcinomas are reported [5]. Malignant odontogenic tumours represent only 1% to 6.1% of all odontogenic tumours. The malignant forms of ameloblastoma are classified into two types: malignant ameloblastoma and ameloblastic carcinoma. Malignant ameloblastoma retains the histological features of benign tumour, but has distant metastasis. Whereas, ameloblastic carcinomas has cellular atypia [6].
Ameloblastomas has very high chance of recurrence if not treated adequately. Curettage is followed by local recurrence in 90% of mandibular and all maxillary ameloblastomas because of insufficient removal of tumors [7]. The current treatment of odontogenic tumours affecting the maxilla is resection with 10-15 mm safety margin of healthy bone. This may include resection of the alveolar ridge, hard palate and maxillary sinus and the lateral nasal wall [8]. Following surgery, close follow up is recommended once a year during the first five years and then every two years with regular CT scan for early detection of recurrence.
Conclusions
Though ameloblastomas are classified as benign tumours, their initial presentation is not different from malignant tumours of maxilla. These tumours can be distinguished from the malignant lesion by imaging studies and by histopathology. The management should be radical to prevent recurrence, similar to malignant lesions. Hence such tumours are better managed in oncology centre where the expertise in surgery, imageology and pathology are present.
References
[1]. Fernandes AM, Duarte EC, Pimenta FJ, Souza LN, Santos VR, Mesquita RA, de Aguiar MC. Odontogenic tumors: a study of 340 cases in a Brazilian population. J.Oral Pathol.Med. 2005 Nov; 34(10):583-7.
[2]. Asaumi J, Hisatomi M, Yanagi Y, Matsuzaki H, Choi YS, Kawai N, Konouchi H, Kishi K. Assessment of ameloblastomas using MRI and dynamic contrast-enhanced MRI. Eur.J.Radiol. 2005 Oct; 56(1):25-30.
[3]. Press SG. Odontogenic tumors of the maxillary sinus. Curr.Opin.Otolaryngol.Head Neck Surg. 2008 Feb; 16(1):47-54.
[4]. Sriram G, Shetty RP. Odontogenic tumors: a study of 250 cases in an Indian teaching hospital. Oral Surg.Oral Med.Oral Pathol.Oral Radiol.Endod. 2008 Jun; 105(6):e14-e21.
[5]. Benlyazid A, Lacroix-Triki M, Aziza R, Gomez-Brouchet A, Guichard M, Sarini J. Ameloblastic carcinoma of the maxilla: case report and review of the literature. Oral Surg.Oral Med.Oral Pathol.Oral Radiol.Endod. 2007 Dec; 104(6):e17-e24.
[6]. Goldenberg D, Sciubba J, Koch W, Tufano RP. Malignant odontogenic tumors: a 22-year experience. Laryngoscope 2004 Oct; 114(10):1770-4.
[7]. Vanoven BJ, Parker NP, Petruzzelli GJ. Peripheral ameloblastoma of the maxilla: a case report and literature review. Am.J.Otolaryngol. 2008 Sep; 29(5):357-60.
[8]. Bozza F, Marcelli VA, Pistilli R, Govoni FA, Marsico C. Maxillary ameloblastoma. Minerva Stomatol. 2006 Apr;55(4):215-22.

