Case Report

Giant cell tumor of tendon sheath involving second metacarpal bone: –a rare case report
*Nagarekha Kulkarni and Phaniraj G
- *Department of Pathology, Vijayanagara Institute of Medical Sciences, Bellary 583104, Karnataka, INDIA
- Thursday, October 24, 2013
- Wednesday, November 20, 2013
- Wednesday, November 27, 2013
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction
Giant cell tumor of tendon sheath (GCTTS) is a benign slow growing tumor with a high incidence of recurrence. Intraosseous metacarpal involvement of GCTTS is an uncommon manifestation of this tumor, but it is well known because of its potentially aggressive local growth. Only few cases are reported in the literature.
Case Report
A 22 years old female presented with pain and swelling over the left hand since 3 months. X-ray findings revealed soft tissue lesion over left second metacarpal. On the radial aspect there was a bony erosion of the second metacarpal involving the cortex of the metacarpal. Tumor along with partial excision of left second metacarpal was removed and sent for histopathological examination. Microscopically an admixture of polygonal and spindle shaped mononuclear cells, xanthoma cells, multinucleated gaint cells in a collagenous, variably hyalinised stroma was seen. The histopathological diagnosis of gaint cell tumor of tendon sheath was made.
Conclusion
To conclude this entity has to be kept in mind when there is a swelling in the metacarpal area.
Key Words
intraosseous, synovial, fibrous histiocytoma
Introduction
Giant cell tumor of tendon sheath (GCTTS) is a benign lesion of uncertain etiology that involves inflammation, trauma, toxin, allergy, clonal chromosomal abnormalities and aneuploidy. Jaffe et al originally described the condition in 1941 [1].It is also called as fibrous histiocytoma of tendon sheath, xanthogranuloma, and benign synovium. Approximately 85% of GCTTS may occur in the fingers, while 12% of tumors are located in the knee, elbow, hip and ankle. GCTTS may occur at any age but most typically occurs between the ages of 30 and 50, with a 2:1 female preponderance [2].One of the most important clinical features is that the symptoms of GCTTS are non- specific. The local recurrence after excision is very high and it has been reported upto 10-20% [3]. Treatment consists of careful local excision, particularly microscopic excision and postoperative radiotherapy. Intraosseous metacarpal involvement of GCTTS is an uncommon manifestation of this tumor, but it is well known because of its potentially aggressive local growth [4].Only few cases are reported in the literature. We report a rare case of localised form of GCTTS involving second metacarpal bone in a 22year old female.
Case Report
A 22 years old female presented with pain and swelling over the left hand since 3 months. The swelling was gradual in onset and progressive in nature. Patient complained of increase in the intensity of pain on doing heavy work. Her past history and family history was insignificant. There was no history of fever, cough, loss of appetite, loss of weight, diabetes and hypertension. On physical examination patient had a diffuse swelling over the dorsolateral aspect of left second metacarpal bone. The swelling was measuring 4X3 cms, firm to soft in consistency, non-tender, skin over the mass was pinchable (Figure 1).

Figure 1: Clinical presentation of giant cell tumor of tendon sheath.
Her vital signs and laboratory investigations was within normal limits as shown in Table1.
Table-1: shows vital signs and laboratory findings
Vital Signs:Pulse Rate: 86/minute
Blood Pressure: 130/80 mm of Hg
Respiratory Rate: 28/minute
Temperature: 38.5oc |
Laboratory
Investigations:
Hb%: 14.2g/dl (normal:12.5-14.5g/dl)
RBC Count: 4.8millions/cmm
(normal:4.5-5.5millions/cmm)
Haematocrit: 44% (normal: 35% to 45%)
WBC Count: 7,800 cells/cmm (normal: 4000 to 11,000/cmm)
Differential Count: Neutrophils: 65%
Lymphocytes: 25%
Eosinophils: 04%
Monocytes: 06%
Basophils: 00%
Serum alkaline phosphatise: 78IU/Lt (Normal:
upto 105 IU/Lt.
Random Blood Sugar: 90mg/dl (normal: 70 to 140mg/dl)
Blood
Urea: 19mg/dl (normal: 5 to 25mg/dl)
Serum Creatinine: 0.8mg/dl
(normal: 0.8 to 1.2mg/dl) |
Serological Investigations
HIV-1& 2: Negative
HBsAg: Negative |
|
Routine Urine Examination:
Albumin: Nil Sugar: Nil
Urine micro: 1-2
pus cells/HPF
|
X-ray findings revealed soft tissue lesion over left second metacarpal. On the radial aspect there was a bony erosion of the second metacarpal involving the cortex of the metacarpal (Figure 2 & 3).

Figure 2: Shows pre-operative x-ray of Giant cell tumor of tendon sheath involving second metacarpal bone

Figure 3: Shows pre-operative x-ray of Giant cell tumor of tendon sheath involving second metacarpal bone
The MRI findings revealed an expansile soft tissue lesion in the diaphysis of left second metacarpal bone. The mass was seen in the medulla and extending exophytically both anteriorly and laterally along the radial aspect. There was a breach in the cortex with a hint of permeation and saucerisation. Distal part of the lesion showed geographic margin. Intense post contrast enhancement was seen. Marrow edema was seen to extend till the base of second metacarpal bone.extensor tendon, median nerve was normal. The radiological diagnosis was aggressive tumor or round cell tumor. Fine needle aspiration cytology findings revealed the features of giant cell tumor of tendon sheath. Patient was posted for surgery. Intraoperative findings revealed a well encapsulated swelling arising from the lumbrical tendons extending upto the bony cortex of the metacarpal (Figure 4).

Figure 4: Shows intraoperative findings of Giant cell tumor of tendon sheath involving second metacarpal bone.
Tumor along with partial excision of left second metacarpal was removed and sent for histopathological examination. The graft was taken from the iliac crest and fixed with a wire. Post-operatively patient was treated with a course of antibiotics and analgesics (Figure 5).

Figure 5: Giant cell tumor of tendon sheath under low power (10X, H/E) :shows an admixture of polygonal and spindle shaped mononuclear cells, xanthoma cells, multinucleated gaint cells in a collagenous, variably hyalinised stroma was seen .
The specimen was received in the histopathology section. Macroscopically the specimen was grey white bit of tissue measuring 4X3X2cms. Three bits were given and the tissue was processed routinely and stained with haematoxylin and eosin (H/E). Microscopically an admixture of polygonal and spindle shaped mononuclear cells, xanthoma cells, multinucleated gaint cells in a collagenous, variably hyalinised stroma was seen . The histopathological diagnosis of gaint cell tumor of tendon sheath was made( Figure 6, 7,8).
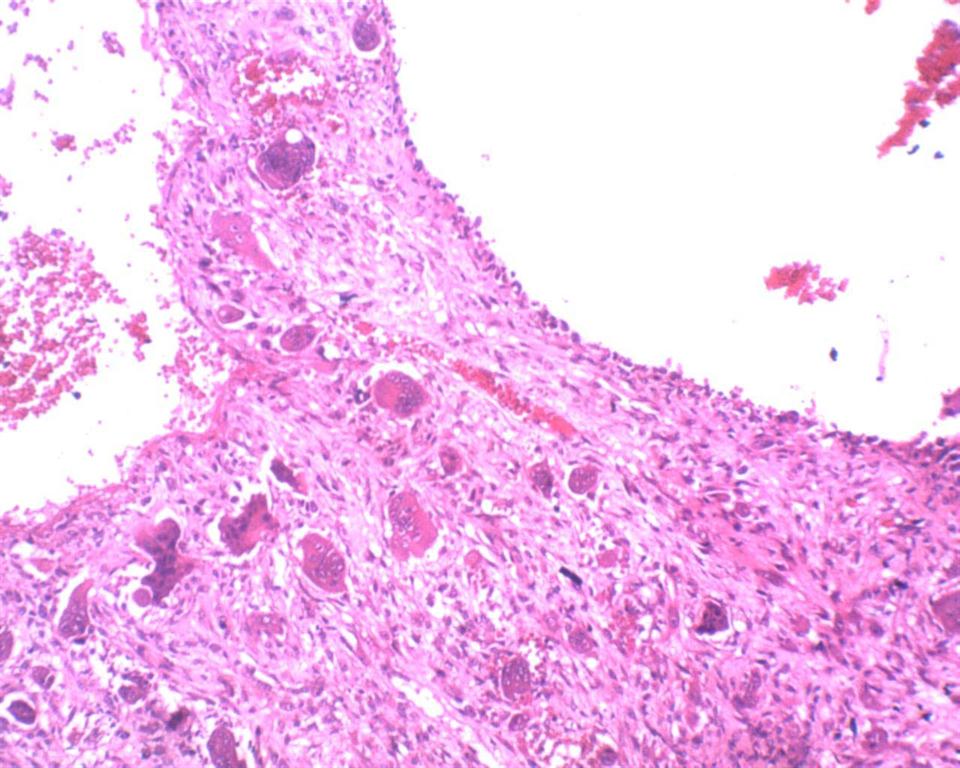
Figure 6: Shows post operative (after 1 week) x-ray of Giant cell tumor of tendon sheath involving second metacarpal bone
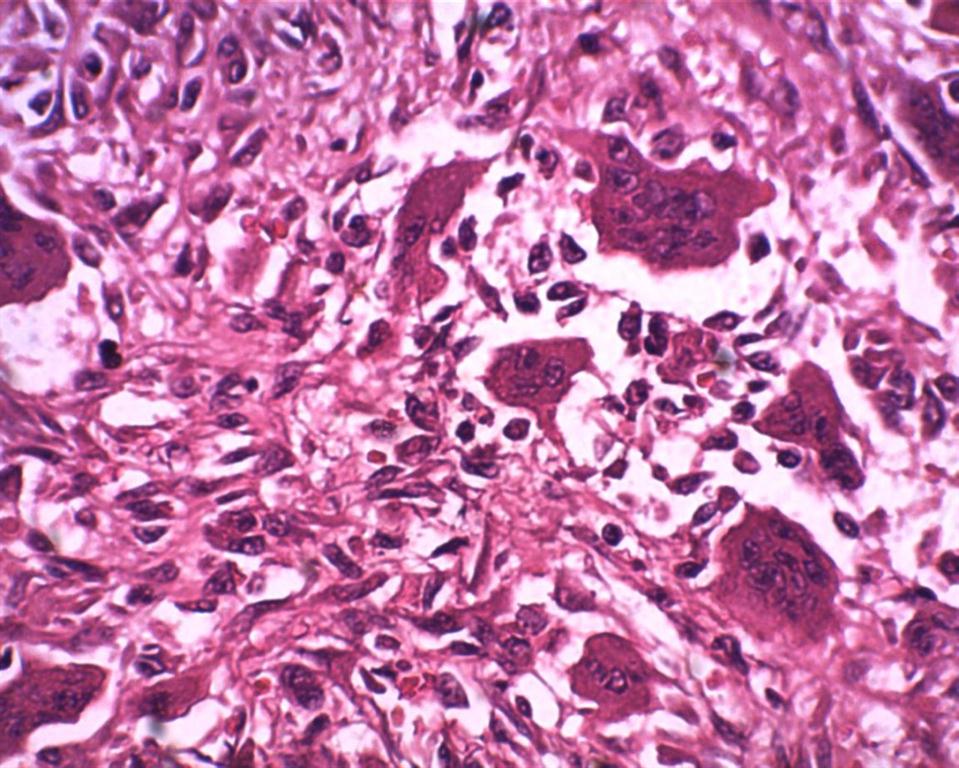
Figure 7: Giant cell tumor of tendon sheath under high power (40X, H/E) :shows an admixture of polygonal and spindle shaped mononuclear cells, xanthoma cells, multinucleated gaint cells in a collagenous, variably hyalinised stroma was seen .
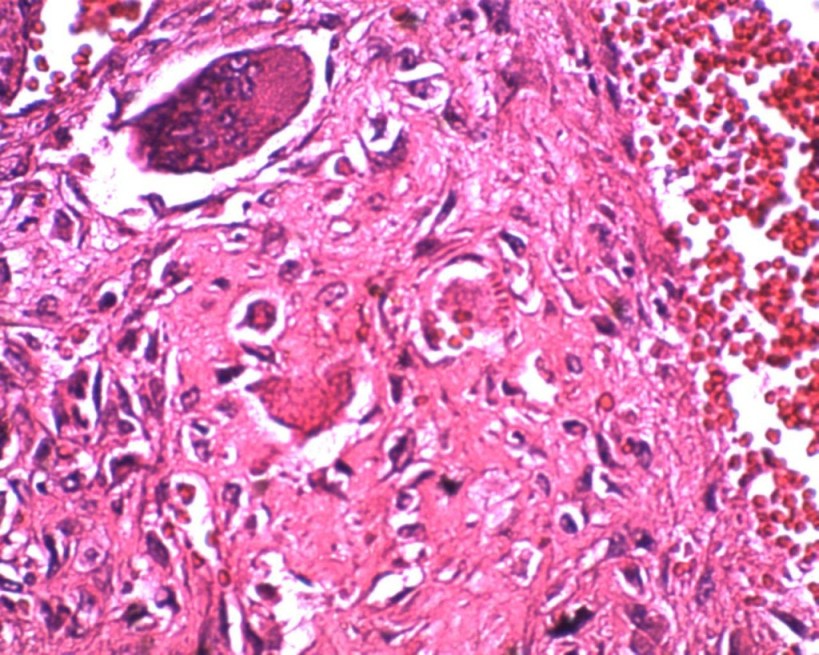
Figure 8: Giant cell tumor of tendon sheath under high power (40X, H/E) :shows an admixture of polygonal and spindle shaped mononuclear cells, xanthoma cells, multinucleated gaint cells in a collagenous, variably hyalinised stroma was seen .
Discussion
The diffuse and localised extra-articular forms of pigmented villonodular synovitis (PVNS) are presently referred to as diffuse-type giant cell tumor and giant cell tumor of the tendon sheath, respectively and were originally alluded to by Jaffe et al in 1941 [1]. The etiology of GCTTS remains uncertain. A variable number of factors have been described as possible causes of GCTTS. These include inflammation, trauma, toxin, allergy, clone chromosomal abnormalities and aneuploidy. GCTTS was initially regarded as an inflammatory disease; however, the finding of aneuploidy in certain cases and the demonstration of clone chromosomal abnormalities strongly support a neoplastic origin [5].GCTTS occurs in the age group of 30-50 years and with a female preponderance. Hand is more frequently involved followed by knee, ankle, wrist and elbow. Prakash et al reported 34.6 years as the average age group with a female preponderance and the distribution of the lesion was more in index finger(16) followed by ring finger (12),middle finger(10), thumb(04), little finger(04),palm(02) in their study of 48 patients[6].Most localised giant cell tumors are small (average tumor size, 2.0 cm), although lesions of greater size may be found in large joints such as the knee and elbow. Tumors are well-circumscribed and typically lobulated, and white to gray in colour, with yellowish and brown areas [5]. This case report shows the involvement of the second metacarpal which is a very rare presentation. Only few cases are reported in the literature. Fogelson MH reported two cases of intraosseous metacarpal involvement of GCTTS [4]. Clinically, GCTTS is a slow growing solitary mass. The mass is painless with discomfort or pain reported in only 20% of tumors. In the present case patient complained of pain on doing heavy work. On plain radiographs, there may be visible soft tissue swelling, sometimes completely encasing the bony elements of the involved digits and the tumor may invade the adjacent bone and cause cystic lesions that are clearly visible on X- ray. 10% involve the bone. In the present case there is involvement of bone. The bone involvement and destruction leads to concern for primary bone malignancy and inappropriately aggressive treatment [7].MRI scans are helpful to define the extent of the lesions and can be helpful in the pre-operative diagnosis. Treatment consists of careful and complete local excision and postoperative radiotherapy. Surgical removal is the standard treatment of GCTTS. Adequate initial local excision may effectively limit the risk of local recurrence [8]. Ikeda et al treated 18 patients with microscopic excision, and of the 18 patients which only one recurred. The reason for this recurrence was that the microscopic excision was not used in the diffuse-type patient. As an adjuvant therapy, postoperative radiotherapy had been indicated to prevent recurrence following surgery [9]. Kotwal et al published a prospective study in which the recurrence rate was only 4%.This rate was much lower than previously published reported incidences of between 25 and 45% [10]. Histopathologically, this lesion contains closely packed medium sized polyhedral cells with a variable admixture of giant cells containing fat and haemosiderin. The differential diagnosis is a very rare malignant counterpart of this lesion chacterised by high number of mitotic figures, marked nuclear hyperchromasia and lack of paucity of multinucleated giant cells. The other differential diagnosis is epithelia sarcoma characterized by the presence of granuloma like formation, necrosis, invasiveness and epitheloid features [11].
Conclusion
GCTCT is a very common tumor in the hand. But involvement of metacarpal is a very rare. This entity has to be kept in mind when there is a swelling in the metacarpal area.
Authors' Contribution
NK: Literature search and preparation of manuscript.
PG:
Preparation of manuscript.
Conflict of Interests
The authors declare that there are no conflicts of interests.
Ethical Considerations
Written informed consent was obtained from the patient for
publication of this case report.
Funding
None Declared
Acknowledgement
None
References
[1]Jaffe HL, Lichtenstein L, Sutro CJ.Pigmented villonodular synovitis, bursitis and tenosynovitis. Arch Pathol.1941; 31:731-765.
[2]Ushijima M, Hashimoto H, Tsuneyoshi M, Enjoji M. Giant cell tumor of the tendon sheath (nodular tenosynovitis): a study of 207 cases to compare the large joint group with the common digit group. Cancer 1986; 57:875-884. [pubmed]
[3]Karasick D and Karasick S. Giant cell tumor of tendon sheath: spectrum of radiologic findings. Skeletal Radiol. 1992; 21(4):219-224.[pubmed]
[4]Fogelson MH, Dao KD, Shin AY. Intraosseous metacarpal involvement of giant cell tumor of the tendon sheath: report of two cases. Am J Orthop (Belle Mead NJ). 2003;32(1):32-4.[pubmed]
[5]Fletcher CDM, Krishnan Unni K, Mertens F, editors. World Health Organization Classification of Tumors, Pathology and Genetics of Tumors of Soft Tissue and Bone. IARC Press; Lyon: 2002. Giant cell tumor of tendon sheath; pp. 110 -111.
[6]Prakash P Kotwal, Vikas Gupta, Rajesh Malhotra. Giant cell tumor of the tendon sheath is radiotherapy indicated to prevent recurrence after surgery.The journal of bone and joint surgery.2000; 82(4):571-573.[pubmed]
[7]www.wheelessonline.com/ortho/giant cell tumor of the tendon sheath.
[8]. Cheng XG, You YH, Liu W, Zhao T, Qu H. MRI features of pigmented villonodular synovitis (PVNS). Clin Rheumatol. 2004; 23:31-34.[pubmed]
[9]Ikeda K, Osamura N, Tomita K. Giant cell tumor in the tendon sheath of the hand: importance of the type of lesion. Scand J Plast Reconstr Surg Hand Surg. 2007; 41:138-142.[pubmed]
[10]. Kotwal PP, Gupta V, Malhotra R. Giant cell tumor of the tendon sheath: is radiotherapy indicated to prevent recurrence after surgery? J Bone Joint Surg Br. 2000; 82:571-573.[pubmed]
[11]Schultz RJ and Kearns RJ. Tumors in the hand. J Hand Surg (Am). 1983; 8(5pt2):803-806.[pubmed]

