Case Report

Carcinoma of the stomach with bilateral adrenal and liver metastasis
1Vinay Kumar, 1Ruhi Dixit, 1Manoj Pandey
- 1Department of Surgical Oncology, Institute of Medical Sciences Banaras Hindu University, Varanasi UP 221005
- Submitted: January 17, 2013
- Accepted: February 18, 2013
- Published: March 23, 2013
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background
Metastatic failures are relatively common in patients who had undergone curative gastric resections. Metastasis commonly occurs to liver and lung, metastasis to other sites is relatively rare.
Case report
This is the first case report in literature of a 48 year male who had underwent radical gastrectomy followed by six cycles of adjuvant chemotherapy with docetaxel and carboplatin. After one and half year, he presented with metastatic disease in liver and bilateral adrenal glands. Capecitabine was started as a single agent. Time to disease progression was six months. On disease progression, erlotinib 150 mg was added to capecitabine. The patient has static disease for one year till he developed multiple liver secondaries and disease progression. The patient was started on weekly paclitaxel with three weekly pegylated adriamycin. After two cycle of chemotherapy the performance status of the patient deteriorated and active treatment was stopped. The patient succumbed to his illness after 3 years 2 months from the date of first diagnosis.
Conclusion
Docetaxel and carboplatin followed by capecitabine and erlotinib as a second line can be used to prolong the survival in case of advanced gastric cancer.
Introduction
Metastatic gastric cancer usually presents with multiple recurrences or peritoneal dissemination where surgical resection is not possible and the disease is often fatal [1]. Gastric cancer is associated with higher incidence of liver and lung metastasis, as compared to adrenal. Palliative systemic chemotherapy is the only option to improve survival and quality of life. We report here on a case of gastric cancer treated by radical gastrectomy and adjuvant chemotherapy that presented later with synchronously liver and bilateral adrenal metastasis with more than 3 year of survival achieved with systemic chemotherapy.

Figure 1: Computerized tomorgraphic scan showing bilateral adrenal metastasis
Case report
In May 2009, A 48 year old male presented with upper abdominal pain and recurrent vomiting for six months duration. The ECOG was 1 and general physical examination revealed only pallor. Abdominal and per rectal examination were unremarkable. Contrast enhanced computed tomography (CECT) scan of the upper abdomen showed circumferential wall thickening (12mm) in pylorus and distal antrum with minimal perigastric fat stranding. Upper GI endoscopy showed circumferential polypoidal mass at the junction of corpus and ant rum with sliding hiatus hernia. Endoscopic biopsy revealed the adenocarcinoma of the stomach (intestinal type). Carcinoembryonic antigen (CEA) was 6.2 ng/ml. Distal radical gastrectomy with Roux-en-Y isoperistalatic gastrojejunostomy was carried out. Postoperative histology showed adenocarcinoma of the stomach (intestinal type) infiltrating the entire thickness of the wall. Margins were free of tumor infiltration. One of 5 lymph nodes showed tumour deposit. The patient was given six cycles of adjuvant docetaxel and carboplatin at three weekly intervals. CECT upper abdomen after completion of six cycles of chemotherapy showed mild thickening of proximal stomach with normal passage of contrast. Patient was asymptomatic for one year when he presented with recurrent pain in right upper abdomen. A CECT was taken that revealed liver and bilateral adrenal masses with sub centimeter periportal and mesenteric lymphadenopathy (Figure 1, 2). Guided FNAC from both the liver and adrenals showed adenocarcinoma deposits. Patient was started on capecitabine, 14 day on 7 day off, cycle. He was symptomatically better till June 2011. Further CECT upper abdomen showed normal anastomotic site but two hypo dense peripherally enhancing lesion in segment VIII and VI of liver of size 5.8 X 5.0 cm, with enlarged periportal lymph node of size 1.4 cm and nodular enlargement of both the adrenal gland suggestive of progressive disease (Figure 3). Erlotinib 150 mg daily was added to the capecitabine. The patient sustained the treatment very well with good performance status. The response of the treatment was evaluated by CECT upper abdomen which showed multiple peripherally enhancing hypodense lesions in right lobe of liver (Figure 4) with bilateral adrenal gland showed relative defined hypodense soft tissue lesion and as cites. Repeated ascetic fluid tapping was done to symptomatically relieve the patient. In purview of further disease progression the options were discussed with the patient and chemotherapy regimen was changed to paclitaxel weekly with 3 weekly pegylated doxorubicin. The patient developed severe grade IV diarrhea and vomiting after 2nd course of the chemotherapy which was managed conservatively His performance status deteriorated in due course, active cancer treatment was stopped and he was put on only supportive treatment. The patient finally succumbed to his illness three years two months after the date of first diagnosis.
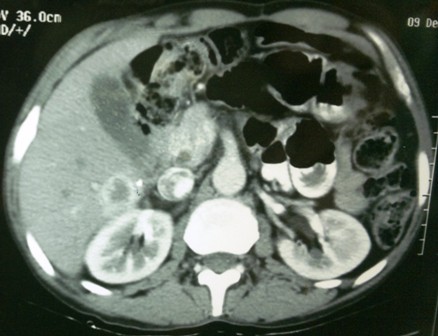
Figure 2: CT scan showing adrenal metastasis with liver metastasis
Discussion
Patients with metastatic gastric cancer have a median survival of 3-5 months with best supportive care. Palliative care in asymptomatic patient’s attempts to improve median survival and quality of life .Gastric cancer with liver metastasis is a non-curable, fatal disease with a 5-year survival of less than 10% [2-5]. In a series of 208 patients, Liver metastases have been reported to be of 13.5% where diagnosis was made within 2 years after surgical treatment. The estimated cumulative risk of liver metastases after 5 years was 16.4%. Preoperative positivity for serum tumour markers, lymph node involvement, and intestinal histotype are risk factors for liver metastases after radical surgical treatment for gastric cancer [6]. Adrenal metastases from gastric cancer are not rare in patients with advanced disease. Metastases from gastric cancer to the adrenal glands occur by direct invasion, a hematogenous route or a lymphatic route.
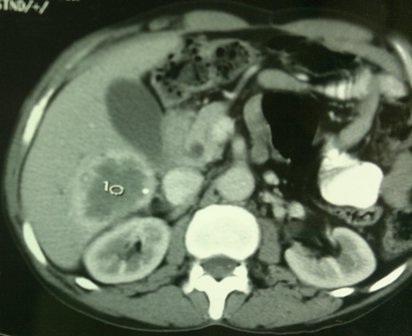
Figure 3: CT scan showing progression of disease.
This is the first report in the literature of carcinoma of stomach with simultaneous liver and bilateral adrenal metastasis with three year survival with the combination chemotherapy. Our patient was treated with potentially curative gastrectomy in spite of giving adjuvant chemotherapy with docetaxel and carboplatin, the patient presented with recurrent disease to liver and bilateral adrenal glands after one year. Adrenal metastasis is found in 16-18 % of the gastric cancer at the time of autopsy [7]. In a study from Korea, recurrence patterns were analyzed in 2,038 patients who were treated with potentially curative gastrectomy. Of 508 patients who developed recurrence, 33% involved loco-regional sites, 44% were peritoneal, and 38% were distant. At time of presentation, 35% of patients present with distant metastasis, with 4% to 14% having liver metastases [8]. There are various reports in literature which have reported long term survivors in carcinoma stomach with distant metastasis [9-10]. A case of 10-year survival after combination chemotherapy of 5'-deoxy-5-fluorouridine and cisplatin and adjuvant surgery for gastric cancer with liver metastasis was reported by chikawa J et al., [11]. Similar report has been published by Okamura H et al., showing a case of multiple hepatic metastases of gastric cancer that showed complete regression by systemic chemotherapy using paclitaxel and UFT-E [12].

Figure 4: Saggital section showing multiple liver metastasis.
Complete response has also been obtained with first-line therapy as S-1, followed by second-line 5'-DFUR plus paclitaxel therapy in a patient with multiple liver and lymph node metastases from gastric cancer [13]. However, in our patient when paclitaxel 100 mg weekly had been used with pegylated adriamycin as a third line chemotherapy, patient develop severe grade IV diarrhea and his performance status deteriorated very fast from which he could not recover. The patient had tolerated the adjuvant docetaxel and carboplatin very well and he had disease free survival of one and half year period. Van Cutsem et al., have reported the use docetaxel in combination with cisplatin and 5-FU in locally advanced cancer stomach [14]. The 2 year survival rate was 18.4% with docetaxel, cisplatin and 5 FU and response rate was 37%. This study had led to the approval of docetaxel by the U.S. Food and Drug Administration for the treatment of gastric cancer when given in association with Cisplatin and 5 FU. We have used the 2 drug combination of docetaxel and carboplatin to avoid the nephrotoxicity and myelosuppression of cisplatin. When the patient developed the liver and adrenal metastasis, capecitabine as a single agent was advised in the palliative setting as per REAL-2 trial [15]. The time to disease progression was 6 months on single agent capecitabine. The patient was started on erlotinib (150 mg daily) and capecitabine combination and he had a stable disease for 11 months before developing disease progression and ascites. Erlotinib has been used in gastric cancer and GE junction cancer but without any known response in gastric cancer, however it has shown a response rate of 9% in GE junction tumor [16]. There has been increased HER 2 positivity has been reported in 6-35% of the gastric cancer. EGFR target has also been evaluated. Cetuximab has been evaluated in phase II trial alone or in combination with FOLFERI [17]. In this limited efficacy trial there was increased response rate but no increase in overall survival. In our patient, we have used erlotinib instead of cetuximab due to poor affordability of the patient and were able to achieve a progression free survival of one year. Thus, in palliative settings the patients should be evaluated for the best available combination chemotherapy to achieve prolonged survival and improves his quality of life.
Conclusion
This is the first report in literature of bilateral adrenal and liver secondaries after potentially curative gastrectomy and adjuvant chemotherapy. The patient has a disease free survival of 1.5 years with the adjuvant chemotherapy with overall survival of three years with erlotinib and capecitabine as a second line chemotherapy. Such chemotherapy regimen of docetaxel and carboplatin followed by erlotinib and capecitabine as a second line could be recommended in advanced carcinoma stomach to prolong the overall survival.
Authors' Contribution
VK: Prepared the draft manuscript.
RD: Did the literature search and helped in preparation of manuscript.
MP: Edited the final version for publication.
Conflict of Interests
The authors declare that there are no conflicts of interests.
Ethical Considerations
Written consent was obtained from the patient for publication of this case report.
Funding
None
References
[1]. Ishii T, Ikegami N, Hosoda Y, Koide O, Kaneko M. The biological behavior of gastric cancer. J Pathol. 1981;134:97–115. [Pubmed].
[2]. Kakeji Y, Maehara Y, Tomoda M, Kabashima A, Ohmori M, Oda S, Ohno S, Sugimachi K: long-term survival of patients with stage IV gastric carcinoma. Cancer 1998, 82:2307-2311. [Pubmed].
[3]. Kumada T, Arai Y, Itoh K, Takayasu Y, Nakamura K, Ariyoshi Y,Tajima K: Phase II study of combined administration of 5-fluorouracil, epirubicin and mitomycin-C by hepatic artery infusion in patients with liver metastases of gastric cancer.Oncology 1999, 57:216-223. [Pubmed].
[4]. Hundahl SA, Phillips JL, Menck HR: The National Cancer Data Base Report on poor survival of U.S. gastric carcinoma patients treated with gastrectomy: Fifth Edition American Joint Committee on Cancer staging, proximal disease, andnthe "different disease" hypothesis. Cancer.2000; 88:921-32. [Pubmed].
[5]. Yagi Y, Seshimo A, Kameoka S: Prognostic factors in stage IV gastric cancer: univariate and multivariate analyses. Gastric Cancer 2000, 3:71-80. [Pubmed].
[6]. Marrelli D, Roviello F, De Stefano A, Fotia G, Giliberto C, Garosi L, Pinto E. Risk factors for liver metastases after curative surgical procedures for gastric cancer: a prospective study of 208 patients treated with surgical resection. J Am Coll Surg. 2004 Jan;198(1):51-8. [Pubmed].
[7]. Cedermark BJ, Blumenson LE, Pickren JW, Elias EG. The significance of metastases to the adrenal gland from carcinoma of the stomach and esophagus. Surg Gynecol Obstet. 1977;145:41–48. [Pubmed].
[8]. Yoo CH, Noh SH, Shin DW, et al. Recurrence following curative resection for gastric carcinoma. Br J Surg 2000;87(2):236-42. [Pubmed].
[9]. Zacherl J, Zacherl M, Scheuba C, et al. Analysis of hepatic resection of metastasis originating from gastric adenocarcinoma. J Gastrointest Surg 2002;6(5):682-9. [Pubmed].
[10]. Sakamoto Y, Ohyama S, Yamamoto J, et al. Surgical resection of liver metastases of gastric cancer: an analysis of a 17-year experience with 22 patients. Surgery 2003; 133(5):507. [Pubmed].
[11]. Chikawa J, Koizumi W, Tanabe S, Takeuchi H, Nagaba S, Higuchi K, Sasaki T, Tahara K, Murakami S, Kitamura T, Nakai H, Saigenji K. A case of 10-year survival after combination chemotherapy of 5'-deoxy-5-fluorouridine and cisplatin and adjuvant surgery for gastric cancer with liver metastasis. Gan To Kagaku Ryoho. 2004 Feb;31(2):255-8. [Pubmed].
[12]. Okamura H, Fujiwara H, Ichikawa D et al . A case of multiple hepatic metastases of gastric cancer that showed complete regression by systemic chemotherapy using paclitaxel and UFT-E. Gan To Kagaku Ryoho. 2009 Jun;36(6):987-90. [Pubmed].
[13]. Kitajima Y, Yakabe T, Ohtsuka T, Tanaka M, Sato S, Nakafusa Y, Miyazaki K. Complete response obtained with first-line therapy as S-1, followed by second-line 5'-DFUR plus paclitaxel therapy in a patient with multiple liver and lymph node metastases from gastric cancer. Gan To Kagaku Ryoho. 2009 May;36(5):851-4. [Pubmed].
[14]. Van Cutsem E, Moiseyenko VM, Tjulandin S, et al. Phase III study of docetaxel and cisplatin plus fluorouracil compared with cisplatin and fluorouracil as first-line therapy for advanced gastric cancer: a report of the V325 Study Group. J Clin Oncol 2006;24(31):4991-7. [Pubmed].
[15]. Nardi M, Azzarello D, Maisano R, et al. FOLFOX-4 regimen as first-line chemotherapy in elderly patients with advanced gastric cancer: a safety study. J Chemother 2007;19(1):85-9. [Pubmed].
[16]. Dragovich T, McCoy S, Fenoglio-Preiser CM, Wang J, Benedetti JK, Baker AF, Hackett CB, Urba SG, Zaner KS, Blanke CD, Abbruzzese JL . Phase II trial of erlotinib in gastroesophageal junction and gastric adenocarcinomas: SWOG 0127. J clinical oncol 2006 Oct 20;24(30):4922-7. [Pubmed].
[17]. Pinto C,Fabio F,Barone C ,et al .Phase II study of cetuximab in combination with docetaxel and cisplatin with untreated advanced gastric and gastroesophageal junction carcinoma.Br J Cancer 2009;101:1261-1268. [Pubmed].

