Case Report

Submucosal calcifying fibrous tumor of stomach: a rare case report
1,Jayashree Krishnamurthy, 2Shetty Mahesh Sanjeeva, 1Kakoti Lopa Mudra, 1Nadig Deepak Muralidhara,1, Sowmya Uthaiah, 1Akriti Kashyap
- 1Department of Pathology, JSS Medical college, JSS University, Mysore, India
- 2Department of Surgical Gastroenterology, JSS Medical college, JSS University, Mysore, India
- Submitted Sunday, June 22, 2014
- Accepted:Sunday, August 03, 2014
- Published Sunday, August 03, 2014
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Intrinsic visceral gastric calcifying fibrous tumor (CFT) is a rare benign mesenchymal tumor often noted as an incidental finding. We herein present a case of a 42 year old male who on evaluation for pain abdomen was found to have calculous cholecystitis and the routine upper gastrointestinal endoscopy revealed a submucosal tumor in the distal part of the stomach. Computed tomography scan confirmed the above findings and the sleeve gastrectomy specimen showed a well circumscribed tumor beneath the mucosa. The tumor was composed of dense collagen fibers, fibroblastic spindle cells with areas of hyalinization, scattered psammoma bodies and nodular lymphoid aggregates which were characteristic of CFT. The smaller size, higher age at presentation, with no tendency for local recurrence and the characteristic morphology helps to distinguish gastric CFTs from other sclerosing stromal lesions in this region.
Key words
Submucosa, calcifying fibrous tumor, stomach, psammoma body, lymphoid aggregate
Introduction
Calcifying fibrous tumor (CFT) is a rare, benign mesenchymal tumor that can involve any part of the body but often shows a predilection for the soft tissue and abdominal cavity especially the subserosal location[1 2 3]. Intrinsic visceral CFT is extremely rare with only very few gastric CFTs being reported to date[4]. These tumors are commonly noted as incidental findings and they present as gradually enlarging painless mass[5]. There are no documented sex predominance and the mean age at presentation is 52.5 years with the mean size being 1.9cms [5 6 7]. The smaller size of gastric CFTs with the higher mean age at presentation and no tendency for local recurrence make them not only differ from their other soft tissue counterparts but also suggest that they could have different pathogenic pathways[1]. Morphologically CFT is composed of hyalinized fibrous tissue with interspersed bland fibroblastic spindled cells, scattered psammomatous calcifications and variable prominent mononuclear inflammatory infiltrate [1 2]. We herein present an incidental finding of a CFT in a patient with calculous cholecystitis with cholesterosis.
Case report
A 42 year old male on evaluation for pain abdomen was found to have calculous cholecystitis and on routine upper gastrointestinal endoscopy was seen to have a submucosal tumor in the distal part of stomach [Figure 1] which was further confirmed on computed tomography scan. Sleeve gastrotectomy was done and macroscopically the specimen consisted of a grey pink globular tissue mass measuring 1.5x1.5x1cms beneath an intact mucosa, which on cut section revealed a well delineated firm lesion [Figure 2] Microscopically there was a well circumscribed tumor in the submucosal region of the stomach which was composed of dense collagen fibers and fibroblastic spindle cells in bundles and vague storiform patterns [Figure 3]. The cells had ovoid, bland vesicular nuclei with fine chromatin and they did not show any cellular atypia or mitotic activity. There were areas of hyalinization, many scattered psammoma bodies and nodular lymphoid aggregates [Figure 4] [Figure 5]. With these characteristic features a diagnosis of CFT was offered and the patient on follow is found to have no symptoms or signs of recurrence.

Figure 1: Upper GI endoscopy showing a submucosal tumor

Figure 2: Globular gray white tumor beneath an intact mucosa
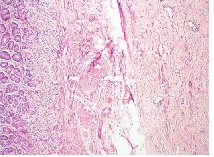
Figure 3: Collagen and fibroblasts in bundles and storiformpattern
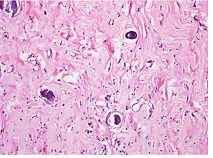
Figure 4: Areas of hyalinization and scattered psammoma bodies
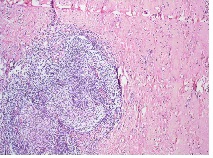
Figure 5: Nodular lymphoid
Discussion
CFTs are benign neoplasms found in ubiquitous anatomical sites including mesentery, peritoneum, mediastinum, pleura, lung, adrenal glands, paratesticular region and the spermatic cord. Rosenthal originally described CFTs as benign soft, fibrous masses with psammoma bodies in the soft tissues of the extremities in children [8]. Although they can involve various organ systems, the gastrointestinal tract is rarely involved and there are only 8 case reports that have described CFTs presenting as submucosal tumors (SMTs) in the stomach and small intestine [3 4 8].
Small SMTs are usually asymptomatic and are incidentally detected during endoscopic or radiological examinations as in the present case. A retrospective study has suggested that the incidence of gastric submucosal lesions is 0.36% and an accurate diagnosis of the SMTs is very difficult based only on endoscopic or radiological findings [8]. A histopathological study of these lesions plays an important role in providing a conclusive diagnosis and can be further confirmed by immunohistochemistry (IHC).
present case is that of a heavily collagenized paucicellular fibrous lesion composed of bland spindled cells arranged in vague storiform pattern with scattered psammomatous and/or dystrophic calcifications, variable mononuclear inflammatory infiltrates and lymphoid aggregates [4 9]. The tumor is often seen in involve the muscularis propria with variable extension into the submucosa and subserosa [4].
Immunohistochemically CFTs show a diffuse positivity for factor XIIIa and negative for CD117, CD34, platelet derived growth factor receptor alpha, S100, smooth muscle actin, muscle specific actin, desmin, anaplastic lymphoma kinase and h-caldesmon [1,4]. Occasional cases have shown focal positivity for CD34 and scattered IgG4-positive plasma cells. Molecular analysis has revealed a wild type for KIT and PDGFRA [4].
The most common differential diagnosis of gastric CFTs include gastrointestinal stromal tumor (GIST), inflammatory fibroid polyp (IFP), schwannoma, sclerosing leiomyoma, inflammatory myofibroblastic tumor (IMT) and plexiform fibromyxoma [7].
Gastric CFTs are distinct from GIST and other mesenchymal gut lesions as they show presence of psammomatous calcifications and lymphoplasmacytic infiltrate as seen in the present case. Gastric GISTs on the other hand are frequently hyalinized with dystrophic calcifications and show immunoreactivity for CD117 and CD34 [10]. Gastric IFPs unlike gastric CFTs are mostly located in the antrum, have higher cellularity, eosinophil dominant inflammatory cells and onion skin pattern of stromal cell arrangement. Gastric schwannomas reveal residual schwannoma tissue and a strong immunoreactivity for S100. Sclerosing leiomyoma has residual smooth muscle tumor cells and show immunoreactivity for both SMA and desmin. It has been postulated that CFT may represent a sclerosing end stage of IMT. Histologically IMT rarely contain calcifications, have infiltrative myofibroblastic proliferation and the inflammatory component is composed primarily of plasma cells and lymphocytes and immunohistochemically IMTs demonstrate diffuse positivity for actin and ALK, variable positivity for CD34 and focal positivity for factor XIIIaPlexiform fibromyxomas are larger tumors of the antrum and have higher cellularity, prominent capillary network, fibromyxoid stroma and show immunoreactivity for SMA [1].The characteristic morphological appearance, the smaller size, higher age at presentation with no tendency for local recurrence helps to distinguish gastric CFTs from other sclerosing stromal lesions of the stomach.
Authors' Contribution
JK: carried out the literature search and drafted the manuscript.
SMS: Operating surgeon and approval of final manuscript for publication.
KLM: carried out the literature search and drafted the manuscript.
NDM: Preparation of the manuscript.
SU: Preparation of the manuscript.
AK: carried out the literature search and drafted the manuscript.
Conflict of Interests
The authors declare that there are no conflict of interests
Ethical Considerations
Written informed consent was obtained from the patient for
publication of this case report.
Funding
None declared
Acknowledgement
None
References
[1].Jang KY, Park HS and Kim CY. Calcifying fibrous tumor of the stomach: a case report. J Korean Surg. Soc. 2012; 83:56-59[Pubmed]
[2].Jang EY, Kim HJ, Kim JH, Lee SO, Choi K and Lee JH. A case of gastric calcifying fibrous tumor presenting as a subepithelial tumor. Korean J Helicobacter Up Gastrointest Res.2013; 13:248-51.
[3].Emanuel P, Qin L, Harpaz N. Calcifying fibrous tumor of small intestine. Ann Diagn Pathol.2008; 12:138-41[Pubmed]
[4].Agaimy A, Bihl MP, Tornillo L, Wunsch PH, Hartmann A, Michal M. Calcifying fibrous tumor of the stomach: clinicopathologic and molecular study of seven cases with literature review and reappraisal of histogenesis. Am J Surg Pathol.2010; 34:271-8
[Pubmed]
[5].Puccio F, Solazzo M, Marciano P, Benzi F. Laparoscopic resection of calcifying fibrous pseudotumor of the gastric wall: a unique case report. Surg Endosc. 2001; 15:1227[Pubmed]
[6].Elpek GO, Kupesiz GY, Ogus M. Incidental calcifying fibrous tumor of the stomach presenting as a polyp. Pathol Int.2006; 56:227-31.
[Pubmed]
[7].Attila T, Chen D, Gardiner GW, Ptak TW, Marcon NE. Gastric calcifying fibrous tumor. Can J gastroenterol. 2006; 20:487-89[Pubmed]
[8].Ogasawara N, Izawa S, Mizuno M, Tanabe A, Ozeki T, Noda H et al. Gastric calcifying fibrous tumor removed by endoscopic submucosal dissection. World J Gastrointest Endosc. 2013; 5:457-60
[Pubmed]
[9].Mao RJ, Xiong XP, Shi J, Li QM, Fang HQ. Clinicopathologic features of calcifying fibrous tumor with reappraisal of its histogenesis. Zhonghua Bing Li Xue Za Zhi.2011; 40:683-8.
[Pubmed]
[10].Agaimy A, Wunsch PH, Hofstaedter F, Blaszyk H, Rummele P, Gaumann A, et al. Minute gastric sclerosing stromal tumors [GIST tumorlets] are common in adults and frequently show c- KIT mutations. Am J Surg Pathol. 2007; 31: 113-20[Pubmed]

