Case Report

Pyelonephritis complicating a multicystic dysplastic kidney with ipsilateral megaureter: initial presentation in an adult
1,Sanjay Marwah, 2Nisha Marwah, 1Hem Kant Verma 3Jyotsna Sen,2, Shilpa Garg 2Rachneet Kohli, 1Hardeep Singh
- Department of1Surgery, 2Pathology and3Radiology, Post graduate Institute of Medical Sciences, Rohtak, Haryana, India.
- Submitted Wednesday, July 2, 2014
- Accepted:Tuesday, July 29, 2014
- Published Sunday, August 03, 2014
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Introduction
Multicystic dysplastic kidney (MCDK) is a rare congenital anomaly that usually presents as neonatal abdominal mass. It presents as a unilateral disorder and ipsilateral ureter is atretic. Its presentation in adults is even rarer due to its involution during initial years of life. In present case, an adult patient presented with renal MCDK with ipsilateral obstructed megaureter that led to pyelonephritis.
Case Report
A 55-year-old male presented with loin pain of one month duration. Imaging studies revealed non functioning right kidney with ipsilateral megaureter. The patient underwent right nephroureterectomy and on histopathology, the diagnosis of MCDK with pyelonephritis was made.
Conclusion
MCDK associated with ipsilateral obstructed megaureter is an extremely unusual presentation in adult patients. Association of pyelonephritis with MCDK is even rarer.
Keyword
Multicystic dysplastic kidney, pyelonephritis, megaureter, adult.
Introduction
Multicystic dysplastic kidney (MCDK) represents a severe form of renal dysplasia and is a common differential diagnosis of neonatal abdominal mass. The ipsilateral ureter is usually atretic and the contralateral system has high incidence of vesicoureteric reflux [1 2]. MCDK presenting in an adult patient is rare probably due to frequent involution of the affected kidney during first few years of life [1]. Here we are presenting an unusual case of renal MCDK with ipsilateral obstructed megaureter that led to pyelonephritis in an adult male.
Case report
A 55-year-old man, who was apparently all right, developed right loin pain since one month. The pain was colicky in nature, moderate in intensity and relieved with oral antispasmodics. There was no history of recurrent urinary tract infection or stone disease in the past. On examination, the patient was normotensive and abdominal examination including genitourinary system was normal. A few epithelial cells and 2-3 leucocytes per high power field were seen in urine microscopy. The routine haematological and biochemical investigations including renal function tests were within normal limits.
Ultrasound of the abdomen and pelvis showed a tubular cystic structure seen extending from right renal fossa to pelvis. Right kidney was not visualized separately and left kidney was hypertrophied. sn MR urography right kidney was not visualized. Right ureter was dilated and tortuous till its lower end. . Left kidney was hypertrophic whereas urinary bladder and urethra were normal (Figure 1). DTPA scan showed non obstructed left kidney with good cortical function. Right kidney was practically non-functioning (Figure 2) On cystoscopy, left ureteric opening was normal whereas right ureteric opening was not visualised.
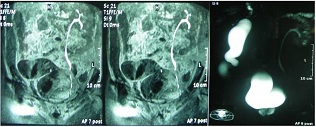
Figure 1: MR urography revealing hypertrophic kidney and normal ureter on left side whereas right kidney is not visualized and right ureter is dilated and tortuous.
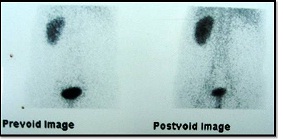
Figure 2: DTPA scan revealing non-obstructed left kidney with good cortical function whereas right kidney is non-functioning.
persistent pain, right nephrectomy was planned. On exploration there was loss of reniform configuration of the kidney which was small in size and resembled a "bunch of grapes"(Figure 3a) The attached pelvis and whole length of ureter were dilated and tortuous till its lower end with obstructed UV junction (Figure 3b). Right renal artery and vein were hypoplastic. Right nephroureterectomy was performed. The cut surface of the kidney showed multiple cystic areas. The creatinin level of fluid collected from the megaureter was 17mg/dl (normal range in urine 20-320 mg/dl) indicating that it was urine only. Histopathological assessment revealed features of classical multicystic dysplastic kidney (Potter type IIA) containing multiple, grapelike clusters of noncommunicating cysts and primitive, poorly branched ducts with smooth muscle collars. There were conspicuous chronic inflammatory changes in form of tubular atrophy, dilation along with thyroidisation of some of the tubules and dense chronic lymphoplasmocytic infiltration of the interstetium that was consistent with chronic pyelonephritis (Figure 4). In megaureter, there was mild inflammation of mucosa and submucosa with thickening of the muscle layer.Post-operative period was uneventful.
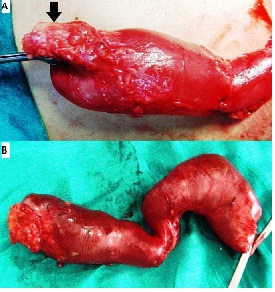
Figure 3: Operative photograph showing small multicystic dysplastic kidney (arrow, 3a) attached to a ureter that is hugely dilated and tortuous along its whole length (3b).
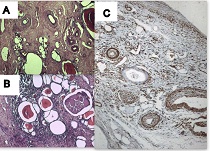
Fig 4: A) Photomicrograph showing variable sized non-communicating cysts surrounded by smooth muscle collar (H&Ex100). B) Areas of chronic pyelonephritic changes showing thyroidisation of tubules and dense interstitial lymphocytic infiltrate (H&Ex100) C) IHC staining showing SMA positive smooth muscle collar around dysplastic ducts and cysts (SMAx100).
Discussion
Multicystic dysplastic kidney (MCDK) is a non genetic, congenital, cystic renal disease in which the cortex is replaced by multiple cysts of variable sizes. Its reported incidence is approximately one in 4300 live births [3]. It is typically a unilateral disorder, since the bilateral condition is incompatible with extra-uterine life. Its proposed mechanism of development is that urinary tract obstruction during embryogenesis leads to failure of the ureteric bud to integrate and branch into the metanephros, with abnormal metanephric differentiation resulting in the de¬velopment of various congenital anomalies in the kidney and urinary tract, including a multicystic dysplastic kidney [4].
The patients with unilateral MCDK commonly have abnormalities in contralateral kidney in form of vesicoureteric reflux, vesicoureteric junction obstruction and pelviureteric junction obstruction [1]. Risdon analyzed clinicopathologic findings of specimens submitted for both nephrectomy and necropsy. He observed that gross cystic renal dysplasia was associated with absence or atresia of the renal pelvis and ureter whereas in patients with segmental renal dysplasia, the ureter was patent and had some anatomical or functional abnormality that resulted in urinary stasis or reflux. Moreover, pyelonephritis was seen in patients with patent ureter and not in patients having atretic ureter [2]. The findings suggested that a lumen was necessary for infecting organisms to gain access to the dysplastic kidney and urinary obstruction was the principal factor leading to pyelonephritis as was noticed in the present case.
The ultrasound appearance of MCDK depends on the age of the patient and it usually shows multiple non-communicating cysts. In a study of 53 children with unilateral MCDK, serial ultrasound performed every six months demonstrated involution of the MCDK with progressive compensatory renal hypertrophy of the contralateral kidney and the involution rate was faster in the first 30 months of life [5]. In adults, DTPA scan is done to assess the function of opposite kidney whereas affected side shows non-visualization of involuted MCDK as was seen in the present case. However, in our case, megaureter was also seen on the side of MCDK as an unusual finding
In the strictest terms, renal dysplasia can be diagnosed only on the basis of histology. When a diffusely dysplastic kidney contains cysts, it is termed a "multicystic dysplastic kidney." Grossly, MCDK may be large or small, reniform or misshapen, and solid or cystic. The classic type (Potter type IIA) contains multiple, grapelike clusters of noncommunicating cysts as was seen in the present case. When the cysts are small or absent, the kidney is said to have solid renal dysplasia (Potter type IIB).The vascular pedicle is hypoplastic and ureter is usually partly or completely atretic. Microscopically, the cysts are lined by low cuboidal epithelium and are separated by thin fibrous septa. Primitive dysplastic elements, especially primitive ducts with smooth muscle collars and immature glomeruli are commonly seen. The presence of primitive ducts on microscopic examination is the hallmark histopathologic lesion of renal dysplasia, although other criteria include primitive glomeruli and nests of metaplastic cartilage [6].Various reports have observed that in most cases, MCDK undergoes involution during the first five years of life [1,3]. However, some patients with nonregression may present in adulthood with renal mass, pain, pressure on adjacent organs and infection [7]. The reasons for advocating nephrectomy of the MCDK are the rare problems of mass effect, infection, hypertension, and potential for malignancy [1]. However, the relation to hypertension and predisposition to malignancy remain undefined possibilities [3 8].
Primary obstructive megaureter is an uncommon presentation in adults. In contrast to its presentation in children, most patients are symptomatic and require aggressive surgical management [9]. Megaureter can be bilateral in 25% of cases, and the contralateral kidney is absent or dysplastic in 10–15% of cases [10]. However, occurrence of primary obstructive megaureter with ipsilateral MCDK and normal contralateral kidney presenting for the first time in an adult is quite unusual. It possibly happened because the right ureteric opening was initially patent and acted as conduit for retrograde transmission of infection leading to pyelonephritis in right kidney. The infection itself might have blocked the right ureter leading to urinary stasis and megaureter. This was the possible reason for delayed presentation of MCDK in an adult patient.
Conclusion
MCDK associated with ipsilateral obstructed megaureter is an extremely unusual presentation in adult patients. Association of pyelonephritis with MCDK is even rarer. Surgical resection is the treatment of choice in such cases.
Authors' Contribution
SM, HKV and HS operated the patient, prepared and reviewed the manuscript.
NM did pathological reporting, drafted and reviewed the manuscript.
JS did radiological work up of the patient, drafted and reviewed the manuscript.
SG, RK, HKV and HS collected the literature, drafted and prepared the manuscript.
Conflict of Interests
The authors declare that there are no conflicts of interests
Ethical Considerations
Written informed consent was obtained from the patient for publication of this case report
Funding
None
Acknowledgement
None
References
[1]Aslam M, Watson AR. Unilateral multicystic dysplastic kidney: long term outcomes. Arch Dis Child 2006;91:820-3. Epub 2006 Jun 5 [Pubmed]
[2].Risdon RA. Renal dysplasia. I. A clinico-pathological study of 76 cases. II. A necropsy study of 41 cases. J Clin Pathol 1971; 24: 57-71.[Pubmed]
[3].Gordon AC, Thomas DF, Arthur RJ, Irving HC. Multicystic dysplastic kidney: is nephrectomy still appropriate? J Urol 1988;140:1231–4[Pubmed]
[4]Pope JC 4th, Brock JW 3rd, Adams MC, Stephens FD, Ichikawa I. How they begin and how they end: classic and new theories for the development and deterioration of congenital anomalies of the kidney and urinary tract, CAKUT. J Am Soc Nephrol 1999;10:2018–28 [Pubmed]
[5].Rabêlo EA, Oliveira EA, Silva JM, Bouzada MC, Sousa BC, Almeida MN, Tatsuo ES. Conserva¬tive management of multicystic dysplastic kidney: clinical course and ultrasound outcome [in Portu¬guese]. J Pediatr (Rio J) 2005; 81: 400–4 [Pubmed]
[6]Minetto M E, Guarnera M P, Arnoletto N. Prenatal Diagnosis of Multicystic Renal Dysplasia (MCRD) or Potter Type II – Report of Two Cases. Hosp Aeronáut Cent 2012; 7: 9-13.
[7].Reitelman C, Becker CJ, Chang C, Perlmutter AD. Infected multicystic dysplastic kidney. Urology 1992; 39: 157-9 [Pubmed]
[8].Birken G, King D, Vane D, Lioyod T. Renal cell carcinoma arising in a multicystic dysplastic kidney. J Paediatr Surg 1985; 20: 619-21.[Pubmed]
[9]Hemal AK, Ansari MS, Doddamani D, Gupta NP. Symptomatic and complicated adult and adolescent primary obstructive megaureter--indications for surgery: analysis, outcome, and follow-up. Urology 2003;61:703-7.
[10]King LR. Megaloureter: definition, diagnosis and management. J Urol 1980;123:222-3 [Pubmed]

