Case Report

Squamous Cell Carcinoma of the Cervix Metastasis to The Jejunum – A Rare Case Report
*Dr. Nagarekha Kulkarni
- Submitted: February 01, 2014;
- Accepted: February 07, 2014;
- Published: February 08, 2014
This is an Open Access article distributed under the terms of
the Creative Commons Attribution License
(http://creativecommons.org/licenses/by/3.0)which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Introduction
Intestinal metastases usually represent a late stage of disease in which other haematogenous metastases are also frequently found. It is exceedingly rare for squamous cell carcinoma of the cervix to metastases to the jejunum.
Case report
This case report describes about a case of 50 years old female presented to the surgical outpatient department with vomiting and pain per abdomen. Resection and primary anastomosis of involved jejunal wall was performed. Diagnosis of peritoneal and jejunal metastases of squamous cell carcinoma associated with mesenteric cyst, adhesion and perforation of jejunum was made.
Conclusion
To conclude, any patient presenting with signs and symptoms of intestinal obstruction it is necessary to keep in mind the possibility of jejunal metastatic tumor and to appropriately diagnose and treat.
Key Words
Perforation, intestinal, resection
Introduction
Metastatic spread to the small intestine is more frequent than to any other site in the gastrointestinal tract. Secondary carcinoma of the small bowel is as common as primary carcinoma at this site. For small intestine, melanoma, lung, breast, colon and kidney are the most frequent primary sites. The pathogenesis of intestinal metastasis usually involves haematogenous spread of tumor cells. Invasion from neighbouring primary tumors also occurs. Examples are pancreatic carcinoma to duodenum and prostatic carcinoma to rectum [1]. Intestinal metastases usually represent a late stage of disease in which other haematogenous metastases are also frequently found. Therefore, the prognosis is poor. Small intestine metastases can present with obstruction, perforation, mal-absorption and haemorrhage. Among these obstruction is the commonest [2]. Small bowel perforation is rarely caused by metastasis from an extra- abdominal malignany. Squamous cell carcinoma of the cervix is the second most common malignancy and majority of the patients usually die from local extension rather than distant metastases. It is exceedingly rare for squamous cell carcinoma of the cervix to clinically present with symptoms related to small bowel metastases [3].
This case report describes about the jejunal metastases from squamous cell carcinoma of the cervix presented with intestinal obstruction.
Case Report
A 50 year old female presented to the surgical outpatient department with vomiting and pain per abdomen since two days. The vomitus contained food material. The pain was diffuse generalised, non-radiating, non-referral. There was no history of diarrhoea, fever, micturition, chills and jaundice. Her significant past history was, she was a known case of carcinoma of the cervix and had undergone abdominal hysterectomy with bilateral salphingo-oopherectomy three months prior to the current presentation. She did not receive any chemotherapy or radiations. Family history was insignificant. Her laboratory investigations and vital signs were normal. The clinical diagnosis was subacute intestinal obstruction. Patient was immediately posted for surgery. Under general anaesthesia midline abdominal skin incision was taken, peritoneum was opened. Jejunum was found attached to anterior abdominal wall besides which jejunal perforation was identified. Resection and primary anastomosis of involved jejunal wall was performed. The resected mass was sent for histopathological examination. Post-operatively patient was observed for 10 days and she was discharged.
The specimen was routinely processed in the histopathology section and stained with haematoxylin and eosin stain (H/E). Macroscopically, the specimen consists of a segment of jejunum measuring 11 cms in length and adherent to the large irregular omental mass (figure-1). The jejunum on the external surface showed presence of two whitish glistening cystic mass on the mesenteric border, the largest measured 3.5 cms in diameter (figure-2).A perforated area surrounded by exudates was seen about 2.5 cms from one of the surgical margin. On cut section entire intestinal lumen appeared normal. The cyst showed presence of serous fluid. The omental mass measured 11 X 6 X 2.5 cms. Cut section showed multiple irregular gray white nodular areas (figure-3). The largest measured 6.5 X 6 X 2.5 cms. Microscopically, the sections from the perforated area showed dense infiltration of polymorphs and haemorrhage. The surrounding mucosa was normal but the submucosa, muscularis and subserosa showed large deposits of metastatic squamous cell carcinoma with central comedo necrosis. Sections from the cyst wall showed features of mesenteric cyst. Sections from the omental mass showed large areas of metastatic deposits of squamous cell carcinoma arranged in epithelial pearls (figure-4, 5). Diagnosis of peritoneal and jejunal metastases of squamous cell carcinoma associated with mesenteric cyst, adhesion and perforation of jejunum was made.
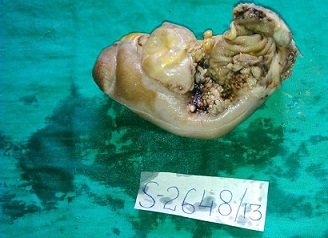
Figure-1: Segment of jejunum measuring 11 cms in length and adherent to the large irregular mass

Figure-2: Jejunum on the external surface show presence of two whitish glistening cystic mass on the mesenteric border

Figure-3: Cut section of large irregular mass show grey white areas
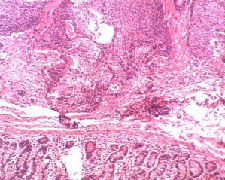
Figure-4: Shows low power view of squamous cell carcinoma metastases to the jejunum (H/E stain)
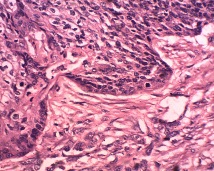
Figure-5: Shows high power view of squamous cell carcinoma metastases to the jejunum (H/E stain)
Discussion
Carcinoma of the cervix usually spreads in an orderly and predictable fashion. The earliest and most common metastases are by direct extension to the contiguous structures including the vagina, peritoneum, and urinary bladder, ureters, rectum and paracervical tissue [4]. However, distant metastatic spread with unusual patterns such as pulmonary lymphangitic carcinomatous has also been reported. Up to 50% of stage IV patients can present with distant metastases. Common sites of such occurrences are the liver, lungs and bone marrow. The gastrointestinal tract is involved in approximately 8% of patients with carcinoma of the cervix and is usually asymptomatic. Isolated metastases to the small bowel are exceedingly rare. Such spread is believed to occur commonly through the lymphatics, usually the para-aortic or mesentric nodes to the bowel’s serosa and less often via the blood stream or by peritoneal seedlings [5].
Extrinsic tumors may involve small intestine by direct invasion, intra-peritoneal seeding or via the haematogenous route [6]. Richie et al suggested intra-luminal seedling of the tumor 5 cells from ingestion of expectorated tumor cells from bronchogenic carcinoma [7]. The tumor emboli usually lodge into the submucosal layer, and their growth typically results in intramural masses with a bulky polypoid extension into the lumen. These polypoid lesions may obstruct the lumen or may ulcerate and present as perforation peritonitis. Sometimes they may ulcerate or erode into a vessel and present as gastrointestinal bleeding [7, 8]. Till today only 8 cases of squamous cell carcinoma metastases to gastrointestinal tract are reported in the literature.
Most of the small bowel metastases present as an emergency. Misonou (1988) reported a case of squamous cell carcinoma with multiple metastases to the small intestine of jejunum presented with symptoms of small intestinal perforation with panperitonitis after 13 years after the primary tumor manifestation [9]. In the present case the patient presented with symptoms of intestinal obstruction like vomiting and pain per abdomen after three months after the primary tumor manifestation. Therefore, it is necessary to pay attention to the symptoms indicative of a metastatic intestinal tumor, such as obstruction, abdominal pain, melena, nausea and so on. The diagnosis is made only at laparotomy. Treatment options in patients with symptomatic small bowel metastases are very limited as their long- term prognosis is very poor. Treatment usually involves local resection of symptomatic lesions and end-to-end anastomosis. Average survival following resection of these tumors is 16 weeks but survival of more than five years has been reported [2]. In the present case resection and primary anastomosis of involved jejunal wall was performed. The prognosis of metastatic intestinal tumor perforation is especially poor. The 1-year survival rate in patients who underwent surgery for the perforation was 12%. It was thought that the prognosis of patients who underwent surgery for a metastatic intestinal tumor was especially poor. In the author’s case the patient died about 2 months after he was transferred to his former hospital (about 3 months after surgery) [4]. In the present case she was observed for 10 days during her post-operative period. Due to poor prognosis and late presentation there is not much literature on their preoperative assessment. Intestinal metastases usually represent a late stage of disease in which other haematogenous metastases are also frequently found. The prognosis is poor.
To conclude any known patient of squamous cell carcinoma of the cervix develop signs and symptoms of intestinal obstruction, it is necessary to keep in mind the possibility of jejunal metastatic tumor and to appropriately diagnose and treat.
Conclusion
None
Authors' Contribution
None
Conflict of Interests
None
Ethical Considerations
None
Funding
None
Acknowledgement
None
References
[1]. Niederau C, Sobin LH. Secondary tumors of the small and large intestine. www.iarc.fr/en/publications/pdfs-online/pat-gen/bb2/bb2-chap4.pdf
[2]. De Castro CA, Dockerty MB, Mayo CW. Metastatic tumors of the small intestines. Surgery Gynecol & Obstetrics. 1957;105:159-65.[pubmed]
[3]. Rani Kanthan, Jenna-Lynn Senger, Dana Diudea and Selliah Kanthan. A review of duodenal metastases from squamous cell cardinoma of the cervix presenting as an 6 upper gastrointestinal bleed. World Journal of Surgical Oncology. 2011;9:113. Doi: 10.1186/1477-7819-9-113.[pubmed]
[4]. Christopherson W, Voet R, Buchsbaum HJ: Recurrent cervical cancer presenting as small bowel obstruction. Gynecologic Oncology. 1985;22:109-114. [pubmed]
[5]. Kanthan R, Senger JLB, Diudea D. Pulmonary lymphangitic carcinomatosis from squamous cell carcinoma of the cervix. WJSO. 2010;8:107. []
[6]. Airoldi M, Gabriele P, Succo G et al. Small bowel metastasis from squamous cell carcinoma of the larynx. A case report. Tumori. 1993;79:286-287.[pubmed]
[7]. Richie RE, Reynolds VH, Sawyers JL. Tumor metastases to the small bowel from extra-abdominal sites. Southern Medical Journal. 1973;66(12):1383-1387.[pubmed]
[8]. Hubens G, Van Eerdeweg W, Schoofs E, Fierens H et al. Massive intestinal haemorrhage due to a solitary jejuna metastasis of a primary bronchogenic tumor. Acta Chir. Beig. 1992;92:87-190. [pubmed]
[9]. Misonou J, Natori T, Aizawa M, Jou B, Tamaki A, Ogasawara M. Stage (Ia) cervical cancer recurring 13 years after hysterectomy and causing small intestinal perforation : a case report with a review of the literature. Acta Pathol Jpn. 1988;38(2):225-34. [pubmed]

