Original Article

Jaw Tumours in Ghanaian Children and Adolescents – A Retrospective Study
Alhassan Emil Abdulai1,Isaac Kwasi Nuamah1,Richard Kwasi Gyasi2
- 1Department of Oral and Maxillofacial Surgery, University of Ghana Dental School, Korle Bu Teaching Hospital, Accra.
- 2Department of Pathology, University of Ghana Medical School, Korle Bu Teaching Hospital, Accra.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction:
There are few reports on the incidence of jaw tumors in the child. Those from Africa mostly originate from Nigeria and tend to dwell on odontogenic tumors only. In the present literature, there are no records describing the incidence of jaw tumors in Ghanaian children. The aim here is to determine the incidence of jaw tumors in children less than 19 years old attending a teaching hospital in Ghana.
Design:
A retrospective study.
Materials and Method:
Histopathological charts at the department of Pathology of a main tertiary healthcare setup between 1989 and 2008 were reviewed and 118 cases belonging to children less than 19 years were studied further. The pathologies were classified and the incidence in each group recorded. All records were analysed using Microsoft Excel spread sheet.
Findings:
92(77.97%) were benign and 26(22.03%) malignant tumors. Male to female ratio for benign was 0.8:1, for malignant was 1.89:1 and for all tumors 0.97:1. 27(29.35%) benign tumors occurred in the maxilla and 65(70.65%) in the mandible. There were 48(40.68%) odontogenic, and 70(59.32%) non-odontogenic tumors. Ameloblastoma was the commonest odontogenic tumour, (30/48) 62.5%. Fibro-osseous lesions (N=31) were the commonest of all the tumors, constituting 26.27% of jaw tumors, and 44.29% of non-odontogenic tumors. Burkitt’s lymphoma was the commonest malignant neoplasm, (17/26)65.38%.
Conclusion:
Most jaw tumors are benign. 19.67%(118/600) affect children and adolescents, Burkitt’s lymphoma is the most prevalent malignancy and together with other non-Hodgkin’s lymphoma form about 20% of all tumors and 88% of all malignancies affecting the jaws in childhood.
Key words:
Jaw tumours; Children; Adolescents; Ghana.
Introduction
The jawbones can be the sites of a multitude of neoplastic conditions [1]. These neoplasms may be benign or malignant. They may also be odontogenic or non-odontogenic. Odontogenic tumors are lesions originating from epithelial and/or mesenchymal components of the tooth-forming apparatus. In children and adolescents, neoplastic lesions are often benign and are of mesenchymal origin [2,3]. Some benign lesions, however, tend to have alarming growth rates, with the tendency to misdiagnose them clinically as malignant lesions, especially in the African population because of the frequent occurrence of Burkitt's lymphoma of the jaws in children [4]. Primary malignant tumors of the mandible and maxilla in children occur less frequently than metastatic or secondary lesions from contiguous or distant sites [5]. When they occur however, the consequences can be severe. Cancer ranks second only to trauma as a cause of childhood mortality in the United States, with about 5% to10% of primary malignancies originating in the head and neck [6].
Reports on the incidence of jaw tumors in children are not many [2,4]. Studies carried out on the subject in Africa have mostly been on odontogenic tumors [6-9]. To the best of our knowledge, there is no published data on the subject among Ghanaian children. Differential diagnosis of these tumors is a crucial part of their management, and to a large extent, depends on our knowledge of them, including their frequency, common sites and histological type. We carried out a retrospective study of 600 histopathological charts on jaw tumors specimens presented to the Department of Pathology of a tertiary healthcare setup, which is the larger of two main referral hospitals in Ghana, over a period of twenty years (1989-2008). We then studied in detail 118 of these reports which met our study selection criteria for patients aged less than 19 years old. The aim of this study is to determine, among others, the incidence, age distribution, localization, and gender preferences of jaw tumors occurring in children less than 19 years. It is hoped that findings from this study will further enhance our understanding of this subject.
Materials and Methods
A retrospective study of the histological records of all jaw tumor specimens of children under the age of 19 years seen at a main Teaching Hospital from 1989 to 2008 (twenty years) was carried out. From a total of 4,546 histopathological reports of head and neck tumors seen at the department of Pathology over the study period, 600 records directly relating to the jaws were selected. Slides of sections were all stained with haematoxylin and eosin. 118 of them belonging to patients who were aged below 19 years were retrieved and studied further. The diagnosis in each case was confirmed and in cases of odontogenic tumors, World Health Organization (WHO) guidelines on classification, (1992) were strictly applied. Parameters of age, sex, site of tumour, the incidence in each group and histopathological diagnosis were documented. All records were analysed using Microsoft Excel spread sheet.
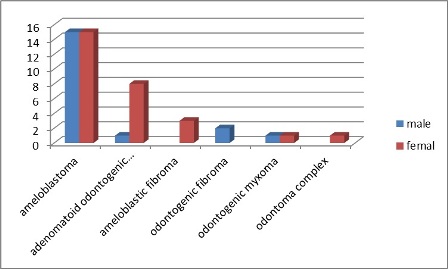
Figure 1: Gender distribution of Odontogenic Tumours
Findings
A total of 600 reports of jaw tumors were recorded over the period of study. From these, 118 met our age selection criteria and were studied in detail. 92(77.97%) were benign neoplasms and 26(22.03%) malignant, (Table1). The male to female ratio for malignant tumors was 1.89:1, for benign 0.8:1 and for all tumors 0.97:1. Twenty-seven, (29.35%) of the benign tumors occurred in the maxilla and Sixty-five (70.65%) in the mandible, (Table2). The commonest was ameloblastoma, N=30 (25.42%). There were forty-eight (40.68%) odontogenic tumors and seventy (59.32%) non-odontogenic tumors, (Table3). The gender distribution of odontogenic tumors is shown in (Figure 1) while that of non-odontogenic in (Figure 2). There was no difference in the incidence of malignancy in both jaws, 13 in each jaw. Predominant malignant neoplasm was Burkitt’s lymphoma, N=17 (14.41%), which had a slight predilection for males and the mandible. In terms of tumor occurrence generally, the mandible was the commoner site, with 78(66.1%) tumors of any kind occurring in it and 40(33.9%) occurring in the maxilla. Some lesions were seen once, demonstrating rarity. The highest incidence of tumors, mainly benign, occurred in the oldest age group stratum, 16-<19 years, (Table 4). However, prevalence of malignancy was highest in the 8-12 age grouping, from where it decreased with increasing age, tending to spare girls and affecting boys only (Figure 3). Over the period of study, the incidence of childhood jaw tumors was 19.67%, (118/600), relative to that of all ages and 2.6 %( 118/4546) relative to all head and neck tumors.
Table 1: Incidence of tumours (Sex and Type)
| Sex |
benign |
malignant |
all tumours |
| Boys |
41
(44.57%)
|
17
(65.38%)
|
58
(49.15%)
|
| Girls |
51
(55.43%)
|
9
(34.62%)
|
60
(50.85%)
|
| Total |
92
(100%)
|
26
(100%)
|
118
(100%)
|
Table 2: Site distribution of Tumours (Benign & Malignant)
| Site |
bening |
malignant |
all tumours |
| Mandible |
65 (70.65%) |
13 (50%) |
78 (66.1%) |
| Maxilla |
27 (29.35%) |
13 (50%) |
40 (33.9%) |
| All |
92 (100%) |
25 (100%) |
118 (100%) |
Discussion
Tumors are part of the spectrum of pathologies seen in clinics managing swellings of the jaws. They are however not common [1]. The World Health Organisation (WHO) classified the various histological types in 1992, [9] revised in 2005 and this has been used worldwide to reclassify jaw tumors. This has served to rationalise the description of these tumors. Differential diagnosis of these swellings is a crucial part of their management [10]. Ruling out the benign from the malignant or aggressive lesion is one of the main aims of most clinicians. Knowledge of the various types of tumors is important in achieving this.
Table 3: Histological diagnosis
| Tumours of the Jaws |
|
|
|
|
|
|
|
| Odontogenic Tumors |
|
|
|
|
|
|
|
| Epithelial Tumors |
|
|
|
|
|
|
|
| Benign: |
Max |
Mand |
Male |
Female |
Total |
%Jaw Tumours |
% Not's |
| Ameloblastoma |
0 |
30 |
15 |
15 |
30 |
25.42 |
62.5 |
| Adenomatoid odontogenic tumor |
6 |
3 |
1 |
8 |
9 |
7.63 |
18.75 |
| Mixed Tumours |
|
|
|
|
|
|
|
| Benign: |
|
|
|
|
|
|
|
| Ameloblastic fibroma |
0 |
3 |
0 |
3 |
3 |
2.54 |
6.25 |
| Odontogenic fibroma |
0 |
2 |
2 |
0 |
2 |
1.70 |
4.17 |
| Odontogenic myxoma/fibromyxoma |
2 |
1 |
2 |
1 |
3 |
2.54 |
6.25 |
| Mesenchymal Tumors |
|
|
|
|
|
|
|
| Odontoma |
0 |
1 |
0 |
1 |
1 |
0.85 |
2.08 |
| Total (Odontogenic Tumours) |
8 |
40 |
20 |
28 |
48 |
40.68 |
|
| Nonodontogenic tumors of the jaws |
|
|
|
|
|
|
|
| Benign: |
|
|
|
|
|
|
|
| Fibro-osseous tumors |
12 |
19 |
14 |
17 |
31 |
26.27 |
44.29 |
| Osteoid osteoma and osteoblastoma |
1 |
0 |
0 |
1 |
1 |
0.85 |
1.43 |
| Osteoma |
0 |
1 |
1 |
0 |
1 |
0.85 |
1.41 |
| cavernous haemangioma |
2 |
4 |
4 |
2 |
6 |
5.08 |
8.45 |
| Angiofibroma |
0 |
1 |
0 |
1 |
1 |
0.85 |
1.41 |
| Neuroectodermal tumour |
2 |
0 |
2 |
0 |
2 |
1.69 |
2.82 |
| Reparative giant cell tumour |
2 |
0 |
0 |
2 |
2 |
1.69 |
2.82 |
| Malignant: |
|
|
|
|
|
|
|
| Teratoma malignant |
2 |
0 |
2 |
0 |
2 |
1.69 |
2.82 |
| Malignant fibrous histiocytoma |
1 |
0 |
1 |
0 |
1 |
0.85 |
1.41 |
| Burkitt’s lymphoma |
7 |
10 |
10 |
7 |
17 |
14.41 |
23.94 |
| Nonhodgkins lymphoma |
3 |
3 |
4 |
2 |
6 |
5.08 |
8.45 |
| Total (Non-odontogenic Tumours) |
32 |
38 |
38 |
32 |
70 |
59.32 |
|
| All Tumours |
40 |
78 |
58 |
60 |
118 |
100 |
|
Of the 118 reports studied, 92(77.97%) were benign and 26(22.03%) malignant. 48(40.68%) were odontogenic tumors (OT) and 70 (59.3%) non-odontogenic tumors (NOT). Miki Sato [12] et al reported 93% incidence of benign tumors in their study.
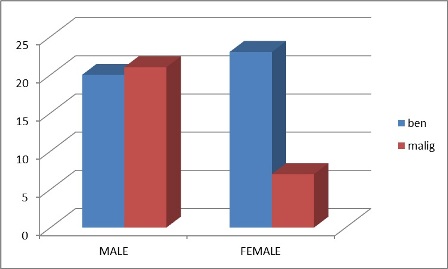
Figure 2: Gender distribution of Non Odontogenic Tumours (benign and Malignant)
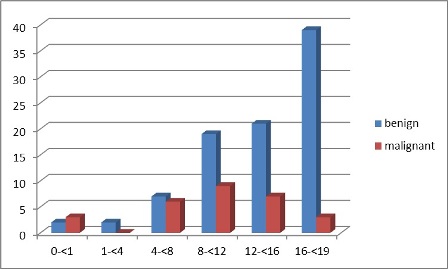
Figure 3: Distribution of tumours by Age Group.
Table 4. Tumour (Odontogenic & non-Odontogenic) Incidence in different Age Groups
| Age |
Benign |
Malignant |
All |
| 0-<1 |
3 |
2 |
5 |
| 1-<4 |
2 |
0 |
2 |
| 4-<8 |
8 |
4 |
12 |
| 8-<12 |
19 |
9 |
28 |
| 12-<16 |
22 |
8 |
30 |
| 16-<19 |
38 |
3 |
41 |
| All Ages |
92 |
26 |
148 |
All the odontogenic tumors seen were benign. There is a wide variation in the incidence of odontogenic tumors reported from different parts of the world. This ranges from 15.9% [3] to 84.8% [12] depending on whether it is expressed as a percentage of the total number of tumors in the selected population or the total number of jaw tumors. In the same country, Nigeria, two studies yielded different figures- 19.3% and 31% [7]. Both of these are lower than our finding. Guerisi
et al., [12] reviewed the literature on this subject and suggested that this may be due to the varied denominators used to determine the rate. The upper limit of the age group varied from 14 years [1]. to 20years [13]. In our study, charts of patients less than 19 years old were selected. The high percentage incidences reported by Sato [13] et al (79.8%), Cohen [14] et al., (83.5%) and Tanaka [11] et al., (84.8%) and the low figures by Ulmansky
et al., [2] (15.9%) and Ajayi et al., [6] (19.3%) lay bare the difficulty in comparing. Adebayo
et al., [7] suggested ethnicity as one possible cause of these wide variations.
As mentioned above, the denominator used to determine the percentage incidence also varies [6,13]. Some authors used the total number of tumors seen in the sample group [6,7] whilst others used the total number of jaw tumors [11,13] This certainly affects the results.
The incidence of benign tumors increased with age in our study (Figure 1). The close relationship between the rises in incidence of benign tumors to increasing age has led some to suggest that these tumors are developmental in origin that tend to enlarge as the patients grow [8,11].
Forty-six of the forty-eight odontogenic tumors (95.8%) occurred from the age of 5 years in this study. This is similar to that reported by Ajayi [6] et al., where most of the tumors (98%) occurred after age 5 years. Al-Khateeb [15] et al., reported 72% of odontogenic tumors in the age group 12-18 years. There is a suggestion in the literature that these neoplasms develop from remnants of the dental lamina or enamel organ during tooth formation [16]. Ajayi [6] suggested the possibility that the formation of these tumors may be linked to the age when crown formation is complete. The commonest site was the mandible (40/48) 83.33%. This is consistent with most reports including those from Africa [7]. However in Al-Khateeb’s study of Jordanian children,[15] the commonest site was the maxilla (64%).
The male female ratio was 20:28 overall with respect to odontogenic tumors. This differs from two other studies from our sub region [6,7], which concluded that boys were more affected. However it is consistent with the study in Israel by Ulmansky
et al., [2]. There is no clear reason for this. The propensity to see more benign tumors in girls and rather less malignant tumors, especially with increasing age has been cited in some other studies [17,18].
The commonest OT was ameloblastoma (30/48). This consists of 62.5% of the OT’s and 25.4% of all the jaw tumors. The youngest patient with ameloblastoma was 7 years old and 29 out of the 30 patients (96.7%) were older than 12 years. All the ameloblastic tumors were seen in the mandible with equal incidence in both boys and girls, (15:15). These findings are similar to other reports from Africa [6,7]. The oncogenesis of ameloblastoma has been strongly associated with the dental lamina and the genetic controls involved in normal tooth formation. The genetic controls take place through several different signaling pathways including bone morphogenetic proteins (BMPs)[16]. This line of research may be the key to unlocking the possible cause of these neoplasms. The strong association of normal tooth development with age may suggest when the signalling pathways are disrupted [16].
The next common OT was adenomatoid odontogenic tumour (AOT) (18.8% of OT’S and 7.6% of jaw tumors). 8 out of the 9 tumors occurred in girls with 6 in the maxilla and 3 in the mandible. The youngest patient with this tumour was 8 years old. These results are similar to the findings of Ajayi
et al., [6] who also reported AOT as the second most common OT, but at variance with reports by Asamoah [1] et al., who reported AOT as the commonest OT amongst Nigerian children. The higher prevalence in females is confirmed in most studies [6,12]. The reason for this is not known.
The third commonest OT’s were ameloblastic fibroma (4.6%) and odontogenic myxoma (4.6% of all OT’s). All the cases of ameloblastic fibroma occurred in the mandible and in girls, whilst the odontogenic myxoma occurred in both jaws (Figure 1). In the general literature this tumour has a slight predilection for boys in the first and second decade. Two of the girls reported here were 15 years old and one 7 years old. The tumour is a mixed odontogenic tumour and has now been separated from other mixed odontogenic tumors as it has been reported to have become malignant in some cases [19].
Four other types of odontogenic tumors were seen, namely, three cases each of ameloblastic fibroma and odontogenic myxoma, two cases (4.2%) of odontogenic fibroma and one case of odontoma, (Table 3). Except the last mentioned, the rest are of mixed (epithelial and mesenchymal) origin. These are rare in African children and adolescents. The finding here is similar to results in other studies,[6,7], but at variance with reports from Japan [13] and Jordan [15] where odontomas are the most common odontogenic tumors and from Israel where Ulmansky
et al., [2] found the commonest OT was odontogenic myxoma amongst children.
There were 70 reports of non-odontogenic tumors (NOT). 32 affecting girls and 38 boys. 44 were benign and 26 malignant. 38 were from the mandible and 32 from the maxilla. The commonest benign NOTs were fibro-osseous lesions (31). They were distributed between the mandible and maxilla in the ratio of 19:12 with a gender distribution of 14:17 (M:F). These findings are akin to that reported by Abdulai
et al., [20] in an earlier study in the same environment, of fibro-osseous lesions in the general population. The next common was cavernous haemangioma (6/70). The others were less common (Table 3).
Of the 26 malignant tumors, 17 affected boys and 9 girls. The incidence peaked in the age group 8-<12 (Figure. 3). The commonest was Burkitt’s lymphoma (17/28) which had a higher incidence in boys than in girls (12:5). Together with other non-Hodgkin’s tumors they consist of 88% (23/26) of all the jaw malignancies. There was also a slight propensity for the lower jaw. From the age of 15 years and above, only boys were afflicted by malignant tumors. The reason for this is not clear and may need investigation. However, similar findings were reported in recent papers by Abdulai, Nuamah
et al., [18] and Gosepath et al., [17].
In both sexes the mandible was the commoner site with respect to all tumors (78:40). This finding is similar to most previous studies. Though there is no established reason for this, genetic factors have been evoked as one of the possible causes of jaw tumors and the formation of the mandible involves more multiple genetic pathways which increases the chances of a genetic process going wrong [16].
The data for this study was from one of the two main referral centres. Though this centre receives referrals from all the ten regions of Ghana a more accurate representation would have been to have a uniform or national centre for collecting data on all pathologies from all the referral centres. There are plans to establish a tumor registry for the whole country. This will help provide a central point for accessing information for studies like this in the future. Also so many patients attend local “medicine men” avoiding the conventional medical care mainly due to their difficult financial circumstances. These constitute the main limitations of this study, as it is difficult to say that the study covered all patients attending hospital or requiring inclusion.
Conclusion
Jaw tumors presenting in Ghanaian children are mostly benign. Fibro-osseous lesions are the most frequent. Ameloblastoma is the commonest odontogenic tumor and Burkitt’s lymphoma is the most predominant childhood jaw tumor. Given the predominance of benign tumors in this study, the need to make the correct diagnosis, based always on histology of surgical specimens cannot be over emphasized.
Authors' Contribution
AEA. conceived and contributed to the design, analysis and data interpretation, drafting and writing the manuscript.
IKN. Contributed to the analysis, interpretation of data and was involved in drafting and writing the manuscript.
RKG Reviewed the histology slides, and contributed to the collection, analysis, and interpretation of the data.
All authors read and approved the final manuscript.
Conflict of Interests
The authors declare that they have no competing interests
Acknowledgement
We wish to acknowledge the secretarial staff of Department of Pathology, University of Ghana Medical School, and Korle Bu Teaching hospital, for their invaluable assistance to us towards retrieving and acquiring data necessary for this work. We thank them most profoundly.
References
[1]. Asamoa EO, Ayanlere AO, Olaitan AA, Adekeye EO: Paediatric tumours of the jaws in Northern Nigeria. J Craniomaxillofac Surg 1990, 18:130-135
[Pubmed]
.
[2]. Ulmansky M, Lustmann J, Balkin N: Tumours and tumor-like lesions of the oral cavity and related structures in Israel children. Int J Oral Maxillofac Surg 1999, 28:291-294 [Pubmed].
[3]. Renner L A, Abdulai A E. Melanotic Neuroectodermal Tumour of Infancy (Progonoma) Treated by Radical Maxillary Surgery. Ghana Med J. 2009 June; 43(2): 90–92[Pubmed].
[4]. Dehner, L. P. (1973), Tumors of the mandible and maxilla in children. II. A study of 14 primary and secondary malignant tumors. Cancer, 32: 112–120. doi: 10.1002/1097-0142(197307)32:1<112::AID- NCR2820320115>3.0.CO;2-D [Pubmed].
[5]. Jay L. Grosfeld. The Plight of Children Ann Surg. 2007 September; 246(3): 343–350 [Pubmed].
[6]. Oluseyi F Ajayi, Akinola L Ladeinde, Wasiu L Adeyemo and Mobolanle O Ogunlewe. Odontogenic tumors in Nigerian children and adolescents- a retrospective study of 92 cases World Journal of Surgical Oncology 2004, 2:39 doi: 10.1186/1477-7819-2-39
[Pubmed].
[7]. Adebayo ET, Ajike SO, Adekeye EO: Odontogenic tumours in children and adolescent: a study of 78 Nigerian cases. J Craniomaxillofac Surg 2002, 30:267-272
[Pubmed].
[8]. Arotiba JT, Ogunbiyi JO, Obiechina AE: Odontogenic Tumours: A 15-year review from Ibadan, Nigeria. Br J Oral Maxillofac Surg 1997, 35:363-367 [Pubmed].
[9]. Kramer IRH, Pindborg JJ, Shear M: WHO Histological Typing of Odontogenic Tumours. 2nd edition. Geneva, Springer-Verlag; 1992.
[10]. Malignant neoplasms of the head and neck. Seminars in Pediatric Surgery: Volume 15, Issue 2, Pages 92-98, May 2006 [Pubmed].
[11]. Tanaka N, Murata A, Yamaguchi A, Kohama G: Clinical features and management of oral and maxillofacial tumors in children. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999 Jul;88(1):11-5
[Pubmed].
[12]. Marcela Guerrisi 1, María Julia Piloni 2, Alicia Keszler Odontogenic tumors in children and adolescents. A 15-year retrospective study in Argentina Med Oral Patol Oral Cir Bucal 2007;12:E180-5 [Pubmed].
[13]. Sato M, Tanaka N, Sato T, Amagasa T: Oral and maxillofacial tumours in children: a review. Br J Oral Maxillofac Surg 1997, 35:92-95
[Pubmed].
[14]. Cohen DM, Bhattacharyya I. Ameloblastic fibroma, ameloblastic fibro-odontoma, and odontoma. Oral Maxillofac Surg Clin North Am. 2004;16:375–84. doi: 10.1016/j.coms.2004.03.005 [Pubmed].
[15]. Al-Khateeb T, Hamasha AA, Almasri NM: Oral and maxillofacial tumours in North Jordanian children and adolescent: a retrospective analysis over 10 years. Int J Oral Maxillofac Surg 2003, 32:78-83 [Pubmed].
[16]. Daiana P. Stolf, Algernon C. Karim and Abhijit G. Banerjee. Genetic aspects of ameloblastoma: a brief review Biotechnology and Molecular Biology Review Vol. 2 (5), pp. 116-122, December 2007
.
[17]. Incidence of childhood cancer of the head J Gosepath, C Spix, B Talebloo, M Blettner, W J Mann and neck in Germany. Annals of oncology official journal of the European Society for Medical Oncology MO (2007) Volume: 18, Issue: 10, Pages: 1716-1721 [Pubmed].
[18]. Abdulai A.E, Nuamah I.K and Gyasi R.K. Head and neck tumours in Ghanaian children - A 20 year review. Int J Oral Maxillofac Surg (2012), http://dx.doi.org/10.1016/j.ijom.2012.06.004
.
[19]. Altini M, Thompson SH, Lownie JF, Berezowski BB. Ameloblastic sarcoma of the mandible. J Oral Maxillofac Surg. 1985; 43:789–94. doi: 10.1016/0278-2391(85)90336-2 [Pubmed].
[20]. Abdulai A. E, Gyasi R.K and Iddrissu M.I. Benign Fibro-Osseous Lesions of the Facial Skeleton - Analysis of 52 cases seen at the Korle Bu Teaching Hospital. Ghana Medical Journal, September 2004, Vol.38,No.3.


