Case Report

A rare case of adrenocortical oncocytic neoplasm presenting with abdominal lump: a case report
1Shashikant Saini, 1Shamsuddin J.Virani, 1Rakhit Shah
- 1Department of surgical oncology, Bhagwan Mahaveer cancer hospital and research centre. Jaipur, Rajasthan
- Submitted:
October 24, 2012
- Accepted:
December 5, 2012
- Published:
December 21, 2012
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Introduction
Oncocytic neoplasms are composed of oncocytic tumor cells, which are characterized by having large, eosinophilic, granular cytoplasm owing to the aberrant accumulation of mitochondria [1]. The most commonly reported sites for oncocytic neoplasms are the Thyroid, kidney and Salivary gland. Oncocytic neoplasms of the adrenal cortex are extremely rare. Most adrenocortical oncocytic neoplasms are benign and non-functioning and are detected incidentally. We report the case of a patient with a non functioning adrenal oncocytic neoplasm who presented with abdominal lump.
Case Presentation
A 40 years old normotensive female presented to our centre with complaints of left sided abdominal discomfort for last 4 months. There were no associated symptoms of fever, pain, anorexia, weight loss or complaints related to bowel or bladder disturbances. She had no features suggestive of any endocrine dysfunction. There was no significant past or personal or family history.
On physical examination a well defined mobile lump could be palpated in left lumbar region.
Routine blood investigations were within normal limits.
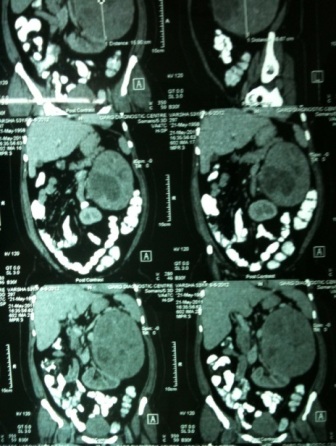
Figure 1: contrast enhanced CT scan of abdomen showing left adrenal mass.
She underwent contrast enhanced CT scan of abdomen , which showed a 15 x 11 square cm mass lesion in the retroperitoneum with areas of focal non enhancing necrotic region and calcification. Mass was located in the left adrenal region, left adrenal gland could not be seen separate from the mass. Mass was pushing left kidney medially and inferiorly and pancreatic tail superiorly. There was no vascular encasement of renal vessels. There was no significant lymphadenopathy (Figure-1).
A functional adrenal tumor was ruled out by, serum catecholamines and 24 h Urinary VMA and serum cortisol, all were within normal range.
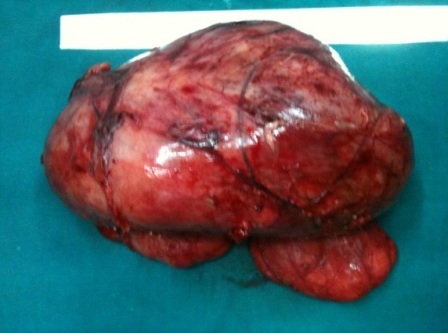
Figure 2: Resected specimen of Left adrenal mass.
She underwent exploratory laparotomy and excision of mass,there was no fluctuation of blood pressure intra-operatively (Figure–2).
Postoperative period was uneventful. Histopathological examination revealed oncocytic arenocortical neoplasm. There was focal necrosis and infarction seen. There was no mitosis or capsular or vascular invasion seen.
Discussion
Oncocytic tumors originating from the adrenal cortex are extremely rare. To date, only 47 cases have been reported, including 24 oncocytomas, 7 oncocytic neoplasms of uncertain malignant potential and 16 oncocytic carcinomas. The patients had a wide age range (27 to 74 years) with a significant female to male predominance. The neoplasms varied in size from 2.2 cm to 15cm. All arises from the adrenal gland with the exception of two cases, which occurred in heterotopic retroperitoneal adrenal tissue [2,3] and all but one case, oncocytic neoplasms were diagnosed incidentally or during investigation for symptoms that were not attributable to the tumor, such as abdominal pain, hematuria, essential hypertension, episodic vomiting, ascites and edema of the lower extremities [4,5]. El-Naggar et al., [6] reported the case of one patient who suffered from abdominal pain caused by tumor infiltration to the adjacent vena cava and liver.
Oncocytic neoplasms of the adrenal cortex were non-functioning with the exception of three cases who were presented with features of cushing’s syndrome [7,8] and virilizing syndrome [9].
Our patient had a non functioning adrenocortical oncocytic neoplasm who presented with abdominal discomfort.
The biologic behavior of adrenocortical neoplasms is usually indolent. A combination of clinical, biochemical and histological features can differentiate benign and malignant adrenocortical tumors. Clinical features such as distant metastases, surgical unresectability and/or invasion of adjacent organs suggest malignant nature of lesion. The Weiss system is the most widely used and accepted histological scheme to distinguish benign from malignant adrenal tumors [10]. According to this system, the presence of four or more of the nine criteria (high mitotic rate, atypical mitoses, high nuclear grade,low percentage of clear cells, necrosis, diffuse tumor architecture, capsular invasion, sinusoidal invasion and venous invasion) indicates a malignant neoplasm. However, the Weiss criteria have limitations. First, Weiss studied only 43 adrenocortical tumors of which 25 were benign and 18 were malignant tumors according to his classification. Second, patients with benign tumors in his series had a longer follow-up period than those with malignant tumors. Third, tumor tissue could be heterogeneous within the same lesion. Therefore, the Weiss score, even if established by experienced pathologists, cannot be completely reliable. Pohlink et al., [11] reported a patient with an adrenal incidentaloma, which was initially diagnosed as benign but on follow-up was reclassified as malignant because of local recurrence and pulmonary metastases.
Bisceglia et al., [12] proposed new criteria that modified the Weiss system. According to this system, if the tumor exhibits any of the major criteria (high mitotic activity, atypical mitoses or venous invasion), it is considered malignant; if the tumor exhibits any of the minor criteria (large size, necrosis, capsular or sinusoidal invasion), it is considered to have uncertain malignant potential; and none of these features indicates a benign tumor [12]. Therefore, this case was diagnosed as oncocytic neoplasm with uncertain malignant potential according to the system proposed by Bisceglia et al.
Adrenocortical oncocytomas are generally considered as benign neoplasms. In 22 of the 25 reported patients for whom follow-up information was available, no recurrence or metastases were observed within a follow-up period ranging from 1 to 99 months.
Borderline adrenal oncocytomas also seem to have a benign clinical behavior. Bisceglia
et al., [12] reported four patients with a mean follow-up of 38.75 months (10 to 61 months) with no evidence of the disease. Lin et al., [5] reported two patients with uncertain malignant potential with a mean follow-up of 15.5 months (12 to 19 months) who had not experienced recurrence or metastases.
Recurrence and metastases have been described in patients with an adrenal oncocytic carcinoma. Kurek et al., [13] described a patient who exhibited widespread retroperitoneal infiltration 7 years after the removal of an adrenal tumor. Local invasion into the inferior vena cava and extension to the right atrium was observed in one case and to the liver in another.
There was no evidence of metastases in our patient. The tumor was compatible with the diagnosis of an oncocytic neoplasm with uncertain malignant potential. The mass was surgically removed and no other therapy was given. After 6 months of surgery patient is still alive without evidence of recurrence and metastases. The patient will be followed-up to check for any recurrence or metastases every 4 months.
Conclusion
Although rare, adrenocortical oncocytic neoplasms must be considered among the differential diagnosis of both functional and non-functional adrenal masses. Clinical, biochemical and histological features must be evaluated together to assess the biologic behavior of these tumours.
Abbreviations
VMA: Vanillyl Mandellic Acid.
Authors' Contribution
SS, SJV: Concept, editing and review of manuscript.
SJV: Design and Literature search of manuscript.
SS, SJV, RS: Definition of intellectual content of manuscript.
SJV, RS: Manuscript preparation.
SS: Guarantor of manuscript.
Conflict of Interests
The authors declare that they have no competing interests.
Ethical Considerations
Case reports can be good science. Good science is by necessity predicated on a respect for best ethical practice. Such respect should not be perceived as a barrier to science, and, should be considered a precondition of scientific practice.We had taken informed consent for case report publication and ensure further confidentiality.
Funding
If my manuscript is accepted, I will pay by credit card, cheque, purchase order, or institutional invoice, using personal, grant or institutional funds.
References
[1]. Chang A, Harawi SJ. Oncocytes, oncocytosis, and oncocytic tumors. Pathol Annu. 1992;27:263–304. [Pubmed].
[2]. Nguyen GK, Vriend R, Ronaghan D, Lakey WH. Heterotopic adrenocortical oncocytoma. A case report with light and electron microscopic studies. Cancer. 1992;70:2681–2684. [Pubmed].
[3]. Poretti D, Mazzarol G, Bonomo G, Casadio C, Bellomi M. Adrenocortical oncocytoma: case report. Clin Imaging. 2003;27:426–430. [Pubmed].
[4]. Krishnamurthy S, Ordóñez NG, Shelton TO, Ayala AG, Sneige N. Fine-needle aspiration cytology of a case of oncocytic adrenocortical carcinoma. Diagn Cytopathol. 2000;22:299–303. [Pubmed].
[5]. Lin BT, Bonsib SM, Mierau GW, Weiss LM, Medeiros LJ. Oncocytic adrenocortical neoplasms: a report of seven cases and review of the literature. Am J Surg Pathol. 1998;22:603–614. [Pubmed].
[6]. El-Naggar AK, Evans DB, Mackay B. Oncocytic adrenal cortical carcinoma. Ultrastruct Pathol. 1991;15:549–556. [Pubmed].
[7]. Xiao GQ, Pertsemlidis DS, Unger PD. Functioning adrenocortical oncocytoma: a case report and review of the literature. Ann Diagn Pathol. 2005;9:295–297. [Pubmed].
[8]. Kabayegit OY et al, Adrenocortical oncocytic neoplasm presenting with Cushing's syndrome: a case report, J Med Case Reports. 2008; 2: 228. [Pubmed].
[9]. Erlandson RA, Reuter VE. Oncocytic adrenal cortical adenoma. Ultrastruct Pathol. 1991;15:539–547. [Pubmed].
[10]. Medeiros LJ, Weiss LM. New developments in the pathologic diagnosis of adrenal cortical neoplasms. A review. Am J Clin Pathol. 1992;97:73–83. [Pubmed].
[11]. Pohlink C, Tannapfe A, Eichfeld U, Schmidt F, Führer D, Paschke R, Koch CA. Does tumor heterogeneity limit the use of the Weiss criteria in the evaluation of adrenocortical tumors? J Endocrinol Invest. 2004;27:565–569. [Pubmed].
[12]. Bisceglia M, Ludovico O, Di Mattia A, Ben-Dor D, Sandbank J, Pasquinelli G, Lau SK, Weiss LM. Adrenocortical oncocytic tumors: report of 10 cases and review of the literature. Int J Surg Pathol. 2004;12:231–243. [Pubmed].
[13]. Kurek R, Von Knobloch R, Feek U, Heidenreich A, Hofmann R. Local recurrence of an oncocytic adrenocortical carcinoma with ovary metastasis. J Urol. 2001;166:985. [Pubmed].


