Case Report

Recurrent Solitary Orbital Neurofibroma: A rare presentation
Rajendra P. Maurya1; Prashant Bhushan1; Virendra P. Singh1; Mahendra K. Singh1; Mohan Kumar2
- 1Department of Ophthalmology, Institute of Medical Sciences, Banaras Hindu University, Varanasi-221 005, (U.P.) INDIA
- 2Department of Pathology, Institute of Medical Sciences, Banaras Hindu University, Varanasi-221 005, (U.P.) INDIA
- Submitted: February 19, 2011;
- Accepted March 11, 2012
- Published: March 28, 2012
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction:
Solitary orbital neurofibromas are rare and chances of their recurrence are remote if completely excised.
Case presentation:
We report here a rare case of unilateral isolated orbital neurofibroma in a nineteen year old male, who presented with large tumor in his right orbit. Complete removal of the mass in medial orbit was performed through medial-transconjuctival orbitotomy. A histopathological diagnosis of neurofibroma was made. Patient was completely symptomless for fifteen years after which recurrence was diagnosed.
Conclusions:
The localized neurofibroma in this case originated from branches of supraorbital nerve and neurofibroma should be considered in the differential diagnosis of orbital tumors of young adult
Introduction
Orbital tumors have always been a diagnostic challenge to the ophthalmologists. Neurofibroma is a benign, peripheral nerve sheath tumor. Neurofibromas of the orbit may be of three subtypes like plexiform, diffuse and localized neurofibromas. Localized neurofibromas of the orbit are relatively uncommon. Symptoms and signs of localized orbital neurofibromas depend on its location in orbit. Its clinical presentation are similar to the orbital schwannomas and present as a localized orbital mass with slow progressing painless or mildly painful proptosis in young to middle aged adults. An unusual case of recurrent localized orbital neurofibroma arising in superomedial orbit, diagnosed on histopathology is being described.
Case Report
A 19-year old male presented with a painless slowly growing mass in the right medial side of the orbit with progressive diminution of vision for the past four years. There was no history of trauma, surgery, fever and systemic involvement. He had no complain of diplopia or field defects. On examination, visual acuity in right eye was 6/60, unaided. In right eye a solid nontender mass in medial side of orbit was seen, which became more prominent on applying pressure on the lower part of the globe. The size of the mass did not vary with valsalva maneuver, ocular movement or posture. The mass was non-pulsatile and transillumination was negative. There was downward and outward globe displacement/proptosis and ocular mobility was restricted in medial and superomedial direction. The pupillary reactions, color vision and visual fields were normal. Corneal sensations were intact. All the cranial nerves were normal and neurological examination were within normal limits. Slit lamp and fundus examination revealed normal anterior and posterior segments. The left eye examination and general physical examination were within normal limits (Figure 1).

Figure 1: Clinical photograph (a-d) Preoperative photograph showing proptosis with downward and outward displacement of globe. (e-h) Postoperative photograph with absence of proptosis
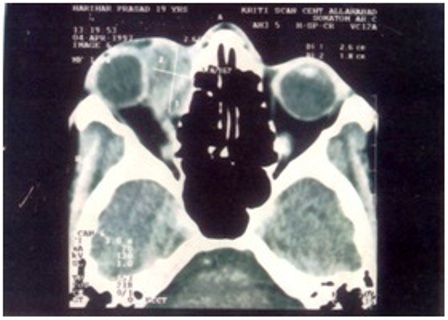
Figure 2 Preoperative orbital computed tomography (CT) scan showing right eye ball compressed and displaced downward and outward due to oval shaped mass (2.6 x 1.8 cm) supero-medially

Figure 3: (A) Peroperative photograph showing trans-conjuctival orbitotomy; (B) Immediate postoperative photograph
Computerized tomography imaging revealed a large (2.6 x 1.8cm), superomedial, solid orbital tumor. The tumor had its origin from the retrobulbar area, extending upto the upper and medial orbit and then protruding externally, thereby significantly displacing the globe laterally and inferiorly. There was no evidence of intracranial and intranasal extension (Figure 2).
A provisional diagnosis of orbital dermoid was made and the patient was taken up for an excision biopsy under general anesthesia. Medial-transconjunctival orbitotomy was performed. Special care was taken to preserve the muscles and the globe. The mass was removed enblock (Figure 3). Peroperative findings were of a smooth, well circumscribed mass with no attachments to the surrounding muscles. None of these structures were infiltrated by the tumor. Postoperatively, patient had a smooth recovery (Figure 1). On follow up after six months vision in right eye was 6/36.
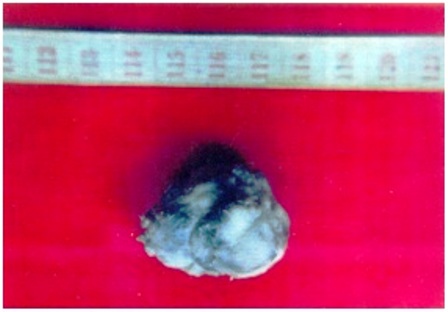
Figure 4: Gross appearance of the excised mass.
On histopathological examination the specimen consisted of a single, nodular, whitish gray, solid mass measuring 3 cm in the greatest diameter. Its cut surface was homogeneous, smooth and gray-white (Figure 4). Microscopically it was diagnosed as a case of neurofibroma giving positive staining with S-100 protein (Figure 5).
Discussion
Neurofibromas are tumors of neurogenic origin. Neurofibromas of orbit are rare and account for 0.6-2.4% of all orbital tumors [1,2]. Histologically, neurofibromas differ from schwannomas, which are pure proliferation of Schwann’s cells, endoneural fibroblast, perineural cells and peripheral nerve axon [3] but from clinico-radiological point of view, localized orbital neurofibroma present like Schwannoma. It presents as a slow growing, solitary, soft tissue orbital mass in young to middle aged adults [3,4,5]. The clinical presentation usually depends on the origin and location of the tumor in orbit. The most common site of localized neurofibromas is superior orbit but may also present in inferior orbit [3,6]. Large neurofibroma of sensory nerves can produce mild to moderate pain which usually disappears after excison of the tumor [5].
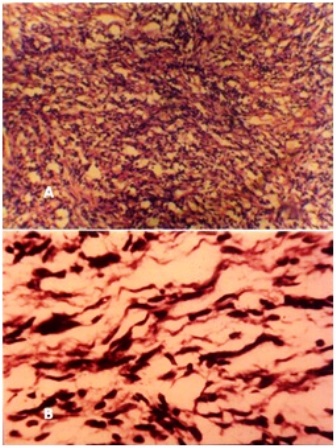
Figure 5: Photomicrograph (A: H and E 40 x) and (B: H and E 100 x) showing neural cells having wavy nuclei in loose fibrillar background
Localized neurofibroma is relatively well circumscribed and much less vascular, unlike plexiform and diffuse neurofibroma which are more vascular and diffusely involve orbital tissues [1,3,5]. There is some controversy regarding capsulation of localized neurofibroma. Although they are encapsulated but they usually can be dissected free from the surrounding tissues and do not recur after complete excision [5,7,8,9,10,11].
Recurrence and re-growth is common with plexiform orbital neurofibroma but not with solitary neurofibroma. In our case, recurrence was diagnosed fifteen years after complete excision. (figure 6). This is the only rare case reported by Gregary of solitary neurofibroma [5]. It may be due to the fact that extremely small neurofibroma get missed or due to transaction of the involved nerve during surgery produces amputation neuroma [5,9].
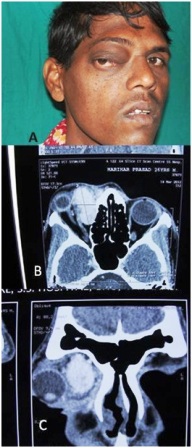
Figure 6: Clinical photograph and CT scan showing late recurrence.
Conclusions
We believe that the localized neurofibroma in this case originated from branches of supraorbital nerve and neurofibroma should be considered in the differential diagnosis of orbital tumors of young adult. Complete surgical excision taking special care of ocular motor nerve is the treatment of choice. Long term follow up is necessary for early detection of possible recurrence or new tumors.
Authors’ Contributions
RPM : Performed literature search, carried out the study and prepared draft and manuscript.
PB : Performed literature search and conducted the study .
VPS : Collected, interpreted and analysis of the clinical data.
MKS :Analysis and interpretation of the data. Read and reviewed the final manuscript.
MK : Collection, interpretation and evaluation of pathological data.
Acknowledgement
We wish to thank Dr. P.R. Sen, Senior Medical Officer, USHCC, Banaras Hindu University for drafting the manuscript and revising it critically and Dr. O.P. Upadhyay, CMO/Ic for helping in the study.
Conflict of Interest
The authors declare that there are no competing interests (conflict of interest).
Ethical Considerations
Written informed consent was obtained from the patient for publication of this case report.
References
[1]. Jakobiec FA, Jones IS : Neurogenic tumors. IN Duane TS (ed) : Clinical Ophthalmology, Vol. 2 Philadelphia. IB Lippincott, 1976.
[2]. Kuo PK, Ni C, Seddon JM, Liu BF, Chen Y : Orbital tumors among Chinese in the Shangai area. Int. Ophthalmol. Clin 1982; 22: 87-98.
[3]. Levin LA, Jakobiec FA: Peripheral Nerve Sheath Tumors of the Orbit, In Fletcher CDM edit Diagnostic histopathology of tumors volume 2; Chapter 242. Elsevier Health Sciences, Philadelphia 2007
[4]. Capps DH, Brodsky MC, Rice CD, Mrak RE, Glasier CM, Brown HH. Orbital intramuscular schwannoma. Am J Ophthalmol. 1990; 110(5):535-539.
[5]. Krohel GB, Rosenberg PN, Wright JE, Smith RS. Localized orbital Neurofibromas. Am J Ophthalmol 1985;100(3):458-64.
[6]. Della Rocca RC, Roen J, Labay GR, Bedrossian E. Isolated neurofibroma of the orbit. Ophthalmic Surg. 1985;16(10):634-638.
[7]. Woog JJ, Albert DM, Solt LC, Hu DN, Wang WJ. Neurofibromatosis of the eyelid and orbit. Int Ophthalmol Clin 1982;22(3):157-87.
[8]. McDonald P, Jakobiec FA, Hornblass A, Iwamoto T. Benign peripheral nerve sheath tumors (neurofibromas) of the lacrimal gland. Ophthalmology 1983; 90(12): 1403-13.
[9]. Blodi, FC : Amputation neuroma in the orbit. Am. J. Opthalmol. 1949; 32: 929-932 :.
[10]. Chua CN, Alhady M, Ngo CT, Swethadri GK, Singh A, Tran S. Solitary nasal neurofibroma presenting as compressive optic neuropathy. Eye 2006; 20(12): 1406-1408.
[11]. Dailey RA, Sullivan SA, Wobig JL. Surgical de bulking of eyelid and anterior orbital plexifor neurofibromas by means of the carbon dioxide laser. Am J Ophthalmol 2000;130(1):117-119


