Case Report

Histopathologic &Immunohistochemical Diagnosis of Primary Epithelioid Angiosarcoma of the Liver Mimicking a Metastatic Adenocarcinoma– Case report & Review of Literature
*, Hema Aiyer * Gaurav Sharma,
- * Anatomic Pathology, Dr Lal Path Labs ;New Delhi, , New Delhi-110085, India
- Submitted Thursday, May 08, 2014
- Accepted:Sunday, October 05, 2014
- Published Saturday, October 25, 2014
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Primary hepatic angiosarcoma is a rare disease with a poor life expectancy. It is believed to be highly lethal, with near 100% mortality by one year. We report a case of a 58 year male who presented with abdominal pain and was incidentally diagnosed as having multiple liver nodules on CT scan suggestive of a tubercular lesion or a lymphoma. Primary histologic examination showed features suggestive of a metastatic adenocarcinoma due to multifocal distribution, epithelioid morphology and presence of lumina. The diagnosis of primary hepatic epithelioid angiosarcoma was finally made following immunohistochemistry which showed positivity for vascular markers.
Key-words
Epithelioid Angiosarcoma, Liver, Mesenchymal malignant tumor
Introduction
Hepatic angiosarcoma is a very rare disease, accounting for only 2% of primary liver malignancy [1 2]. It has a rapidly fatal course where patients usually die within six months of disease onset. Hepatic angiosarcoma originates from endothelial cells and usually presents as an abdominal mass with nonspecific symptoms and signs. Epithelioid angiosarcoma is a morphological variant of angiosarcoma. It occurs in approximately 20% of all angiosarcomas [3]. Epithelioid morphology distinguishes this variant and vascular channel formation typical of angiosarcoma may be scarce or even entirely absent. The correct morphological diagnosis of epithelioid angiosarcoma may be difficult. We present a case of a 58 years old male with primary hepatic epithelioid angiosarcoma with review of literature.
Case Presentation
A 58 years-old male presented to the gastroenterology clinic with complaints of mild abdominal discomfort, anorexia and unexplained weight loss. He had been having these complaints for a few months. On abdominal examination there was tenderness in the right hypochondrium with mild hepatomegaly. Rest of the systemic examination was unremarkable. Laboratory tests were performed and all were non-contributory. CT scan of the abdomen revealed multiple hypodense lesions in both lobes of the liver. Rest of the imaging was normal and there were no other such lesions elsewhere. A possibility of lymphoma or tuberculosis was suggested on imaging. An image guided Trucut liver biopsy was performed. We received 4 linear tissue cores measuring 0.6 to 1.4 cm each.
Histopathologic examination showed liver tissue infiltrated by a neoplastic lesion composed of atypical cells with enlarged hyperchromatic nuclei(Figure 1A)The cells were spindle to epithelioid in shape with abundant cytoplasm, vesicular nucleus and prominent nucleolus in some. Prominent intracytoplasmic vacuoles were seen in many tumor cells (Figure 1B) Tumor cells were forming rudimentary lumina and vascular channels, focally (Figure 1C) The tumor cells showed high grade nuclear atypia and showed brisk mitotic activity and necrosis (Figure 1D&1E).
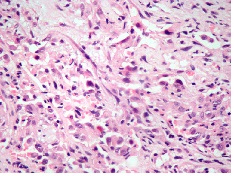
Figure 1A-Solid sheets of tumour cells with marked atypia -x400-HE
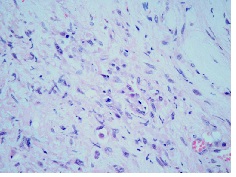
Figure 1B-Intracytoplamic vacuoles in tumour cells x400-HE
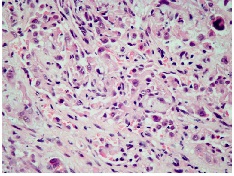
Figure 1C-Slit like sinusoidal vascular channels-x400-HE
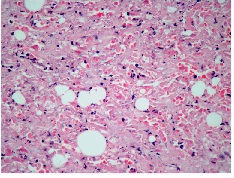
Figure 1D-Extensive tumour necrosis-x400-HE
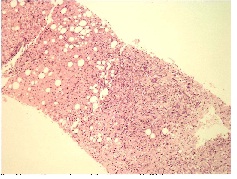
Figure1E- Normal liver parenchyma on left and tumour on right-x100-HE
On immunohistochemistry, the neoplastic cells showed strong diffuse positivity for vascular markers (CD31, CD34) (Figure 1F&1G) and vimentin, and were negative for pancytokeratin, AE1/AE3 ,CD30 and LCA (leucocyte common antigen). Negative immunostaining for Hepatocyte specific antigen (HSA) excluded the possibility of a primary hepatocytic neoplasm In view of histological findings in conjunction with immunohistochemistry, thepossibility of an aggressive vascular neoplasm was considered and the diagnosis of epithelioid angiosarcoma of the liver was given.
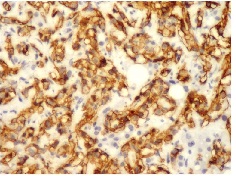
Figure 1F-IHC for CD-34 strongly positive in tumour cells-X400
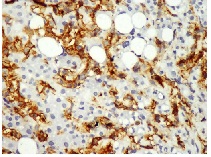
Figure 1G- Diffuse strongCD-31 positivity in tumour cells
Discussion
Angiosarcoma, a subtype of soft tissue sarcoma, is an aggressive malignant disease deriving from endothelium of lymphatics, or blood vessels [4]. Angiosarcoma occurs most commonly in the head and neck, followed by the breast. Liver angiosarcoma is ranked as fifth in the list of commonly seen sites of angiosarcoma and is very rare [5].
Liver angiosarcoma occurs mainly in the elderly. Although the symptoms are usually nonspecific, abdominal distension and discomfort, weight loss, and fatigue are commonly found [6]. Jaundice, ascites and hepatomegaly are usually associated with advanced liver angiosarcoma. In this case the presenting complaints were nonspecific and not very alarming, reflecting an early lesion. The abnormal liver functions found in advanced liver angiosarcoma are attributable to the replacement of normal liver parenchyma by tumor.
There are few reports of multifocal angiosarcomas with epithelioid morphology involving gastrointestinal tract including liver as well as, primary intestinal angiosarcomas with secondary or subsequent liver involvement [6 7.] However in this case, only the liver was involved. Likewise, metastasis from elsewhere was also excluded.
The radiologic findings of hepatic epithelioid angiosarcoma usually pose a diagnostic dilemma for the radiologists. Ultrasonography reveals multiple discrete hypoechoic nodules or a diffusely heterogeneous echotexture of the liver. Computed tomography (CT) scan shows multiple discrete nodules with target appearance or a confluent hypodense mass in the liver. In this case also, it lead to a more common probable diagnosis of either lymphoma or tuberculosis. Hence, a radiologic diagnosis of Hepatic Angiosarcoma may not be possible [8 9].In the absence of classic radiologic features, pathologic examination remains the mainstay of diagnosis of this rare tumor.
Epithelioid angiosarcoma is characterized by epithelioid morphology with scarce or even entirely absent vascular channel formation. Additionally, Epithelioid angiosarcomas express cytokeratins in around 50% of cases (CK was negative in our case) and it makes differentiation from carcinomas more challenging. A strong expression of vascular markers, such as CD31, CD34 and factor VIII are helpful in reaching a correct histopathological diagnosis [10].
Although CD34 shows relatively low immunoreactivity in solid, poorly differentiated areas of Epithelioid angiosarcomas, in our case, the neoplastic cells, although showing strikingly solid morphology, strongly expressed CD34 confirming the vascular nature of the malignancy.
Such solid sheets of mitotically active and markedly atypical tumor cells with extensive areas of tumor necrosis highlight aggressive nature of neoplasm as well as serve to distinguish it from commoner, less aggressive neoplasms like epithelioid hemangioendothelioma, in which prominent cord like pattern of tumor cells in myxo-hyaline stroma is readily evident.
Key Message
Epithelioid Angiosarcoma of liver being rare entity and a morphological mimic of more common entity of adenocarcinoma needs careful evaluation and often immunohistochemical findings for accurate diagnosis
Authors’ contribution
HA: Preparation of manuscript and editing of final manuscript.
GS: Preparation of draft manuscript and literature search
Conflict of Interest
The authors declare that there are no conflicts to declare
Ethical considerations
The authors declare that the written informed consent was obtained from the patient for publication of this case report
Acknowledgement
None
Funding
None declared
References
[1].Mani H, Van Thiel DH. Mesenchymal tumors of the liver. Clin Liver Dis 2001; 5:219-57
[Pubmed]
[2].Molina E, Hernandez A. Clinical manifestations of primary hepatic angiosarcoma. Diag Dis Sci 2003; 48:677-82
[Pubmed]
[3].Deyrup AT, McKenney JK, Tighiouart M, Folpe AL, Weiss SW. Sporadic cutaneous angiosarcomas: a proposal for risk stratification based on 69 cases. Am J Surg Pathol 2008; 32:72-7.[Pubmed]
[4].Locker GY, Doroshow JH, Zwelling LA, Chabner BA. The clinical features of hepatic angiosarcoma: a report of four cases and a review of the English literature. Medicine (Baltimore) 1979; 58:48-64
[Pubmed]
[5].Young RJ, Brown NJ, Reed MW, Hughes D, Woll PJ. Angiosarcoma. Lancet Oncol 2010; 11:983–91.[Pubmed]
[6].Mark RJ, Poen JC, Tran LM, Fu YS, Juillard GF. Angiosarcoma: A report of 67 patients and a review of the literature. Cancer 1996; 77:2400-6.[Pubmed]
[7].Forbes A, Portmann B, Johnson P, Williams R. Hepatic sarcomas in adults: a review of 25 cases. Gut 1987; 28:668-74.[Pubmed]
[8].Buetow PC, Buck JL, Ros PR, Goodman ZD. Malignant vascular tumors of the liver: radiologic-pathologic correlation. RadioGraphics1994; 14:153–66.[Pubmed]
[9].Koyama T, Fletcher JG, Johnson CD, Kuo MS, Notohara K, Burgart LJ. Primary hepatic angiosarcoma: findings at CT and MR imaging. Radiology 2002; 222:667–73.[Pubmed]
[10].Alles JU, Bosslet K. Immunohistochemistry of angiosarcomas. A study of 19 cases with special emphasis on the applicability of endothelial cell specific markers to routinely prepared tissues. Am J Clin Pathol 1988; 89:463–71.[[Pubmed]


