Original Article

Expression of ErbB-1 and ErbB-2 in Cholecystectomy Specimen done for Benign Gallbladder disease
1,Rahat Hadi 2Ashish Singhal 3Shakeel Masood4Namrata P Awasthi
- 11Department of Radiation Oncology,
- 22Department of Surgical Oncology,
- 3Department of Gastro-Surgery,
- 4Department of Pathology, Dr Ram Manohar Lohia Institute of Medical Sciences, Lucknow, India
- Submitted:Saturday, February 01, 2014
- Accepted:Sunday, April 13, 2014
- PublishedMonday, June 16, 2014
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Background Cholecystitis is a common problem in the Indian subcontinent with gallstones as the underlying pathology in majority of patients. Gallstones are also considered as the predisposing factor for gallbladder cancer (GBC), the most common malignancy of the biliary tract (BTC) in India. This pilot study was done to evaluate the expression of ErbB-1 and ErbB-2 in gallbladder specimen removed for cholecystitis (benign disease). The study of these markers in benign disease may serve as a future tool for comparative studies in patients with GBC and evaluate newer targeted therapies for the same.
Method
The present study was done in tertiary care center in north India, in which 11 samples were submitted for ErbB-1 and ErbB-2 evaluation. After performing necessary processing, slides were incubated with primary antibody (ErbB or EGFR) ready to use (RTU) BioGenex, India and ErbB-2 or HER-2/neu dilution 1:600, Dakopatts, Denmark) Then slides were incubated with secondary antibody (Real Envision Detection Kit, Dakopatts, Denmark).Finally in mounted slides, cell membrane staining used to assess positivity for ErbB-1 and ErbB-2.
Results
The data was reviewed on completion of the study, ErbB-1 found to be positive in 7/11(63.64%) patients and negative in 4/11(36.36%) patients. Likewise, ErbB-2 found to be positive in 9/11(81.82%) patients, and negative in 2/11(18.18%) patients.
Conclusions
Cholecystitis and cholelithiasis are two major etiological factors in GBC etiology; it is worthwhile to make efforts in diagnosing GBC in earlier stage. By assessing ErbB-1 and ErbB-2 in Indian scenario and correlating it with GBC, we can make out better plan to handle this deadly disease. Despite the efforts by many investigators, GBC continues to represent a major challenge in oncology. Since this is a pilot study, further larger studies based on molecular understanding are warranted so that new targeted therapies may be developed which may increase the survival of patients with this disease.
Key Words
Cholecystectomy, Cholelithiasis, ErbB-1, ErbB-2, Gallbladder carcinoma, targeted therapy
Background
Despite the recent development in understanding of the cancer biology, the GBC still remains a therapeutic challenge with poor prognosis. High ErbB-1 (EGFR-1) expression, tumor node metastasis (TNM) stage and preoperative serum carbohydrate antigen 19.9 (CA 19.9) are independent predictors of overall survival [1]. Surgery plays a pivotal role in its management with radiotherapy and chemotherapy as adjuncts without much benefit.
ErbB (EGFR) is a protein kinase receptor involved in the signal transduction which affects cellular activities. Increased ErbB expression has been noted in various cancers and has become a useful target for therapeutic interventions. Studies from Asia and Australia have demonstrated ErbB overexpression in GBC with very few studies evaluating the receptor status in inflamed gallbladder which may be a predisposing factor of GBC.
ErbB-2 (HER-2/neu) is protein present in mostly of surface epithelium in large and septal bile ducts and did not correlate to the histopathological grade or tumor stage. Overexpression of the gene product occurs in one forth to about two thirds of BTC and may be used as phenotypic marker for neoplastic transformation with a worse prognosis [2].
Few studies have quoted that no pt. co-expressed ErbB (EGFR) and ErbB-2 (HER-2/neu) [3]. Genomic instability due to Myc amplification may cause specific amplification of ErbB-1 (EGFR-1) and/or ErbB-2 which is found only in 3.7% of the GBC cases but this information might be useful for tailored target therapy in the future [4].
The p53 positivity increased with increasing grade while ErbB-2 positivity decreased with increasing grade of GBC. Mean age in ErbB-2 positive cases were lesser as compared to negative cases, while p53 did not show such association with age. ErbB-2 overexpression in adenoma and younger age group indicates its role as an early event in carcinogenesis of gallbladder [5].
Patients and Methods
The present study was done in tertiary super-specialty
institute of north India. This was a pilot study, and at the time of completion,
11 samples were submitted for ErbB-1 and ErbB-2 evaluation in
post-cholecystectomy patients of cholecystitis, who were meeting the inclusion
criteria (adults, sexes, no associated malignancies or co-morbid conditions and
no prior treatment). The samples were kept in tissue bank having material
adequate for immunohistochemistry (IHC). Consent of the pts., were taken after
explaining the procedure of the study (Table 1,2).
| Patient |
Cholecystitis |
| Total |
11 |
| Age(Years) |
24-65 |
| Median |
50 |
| Male |
3 |
| Female |
8 |
| ErbB-1 Positive |
63.64%(7/11) |
| ErbB-2 Positive |
81.82%(9/11) |
| Status at last Follow Up |
|
| Alive without any disease |
11 |
|
S.
No.
|
Age
|
Sex
|
HPE
|
ErbB-1
|
ErbB-2
|
|
1
|
60
|
F
|
Cholecystitis
|
<10/2+
|
<5/1+
|
|
2
|
65
|
F
|
Cholecystitis
|
Negative
|
Negative
|
|
3
|
52
|
F
|
Cholecystitis
|
Negative
|
Negative
|
|
4
|
45
|
F
|
Cholecystitis
|
<5/1+
|
Negative
|
|
5
|
24
|
M
|
Cholecystitis
|
10/2+
|
<5/3+
|
|
6
|
54
|
M
|
Cholecystitis
|
90/3+
|
70-80/1+
|
|
7
|
53
|
F
|
Cholecystitis
|
>90/2+
|
80-90/2+
|
|
8
|
50
|
F
|
Cholecystitis
|
>90/3+
|
50-60/1+
|
|
9
|
45
|
F
|
Cholecystitis
|
70-80/2+
|
30/1+
|
|
10
|
46
|
M
|
Cholecystitis
|
70-80/3+
|
Negative
|
|
11
|
45
|
F
|
Cholecystitis
|
70-80/2+
|
<5/1+
|
Immuno-histochemical Evaluation
In the pathology laboratory, serial 4 µm sections were cut from the tissue block overnight at 60 °C. De-waxing was done by immersing the warm slides in xylene. After that slides were immersed in graded alcohol 100%, 70%, and 50% and distilled water for 5 minutes. Blocking was done in 50 ml methanol and 1.5 ml H2O2 for 30 minutes and washed with distilled water for 5 minutes. Antigen retrieval was done in pre-warm citrate buffer (pH 6.0) at 90 °C for 90 minutes. Slides were cooled for 30 minutes at room temperature and washed 3 times in Tris-buffer (pH 7.5). Slides were incubated in primary antibody (ErbB or EGFR) ready to use (RTU) BioGenex, India and ErbB-2 or HER-2/neu dilution 1:600, Dakopatts, Denmark)overnight and washed three times in Tris-buffer (pH 7.5) again. Incubate with secondary antibody (Real Envision Detection Kit, Dakopatts, Denmark) for 30 minutes and give 3 washings of Tris-buffer (pH 7.5) and incubate these slides in chromogen (DAB -3, 3’-diaminobenzidine tetra hydrochloride) buffer in 1:50 ratio and give 3 washing of distilled water. Counter the slides with haematoxylin and 3 washings with distilled water and air dry the slides for 15-20 minutes. Finally we mount the slides with DPX mountant. Cell membrane staining is used to assess positivity for ErbB-1 and ErbB-2 (HER 2/neu).
The staining pattern for ErbB-1: Percentage of cells stained: Total number of cells staining positive out of 100 cells counted as an average in 10 high power fields.
0=no staining,
1+= distinct membrane staining visible at 40X magnification only
2+= distinct membranes staining visible at 10 X magnification only
3+= distinct membranes staining visible at 5X magnification only
The staining pattern for ErbB-2 (HER- 2/neu): Percentage of cells stained: Total number of cells staining positive out of 100 cells counted as an average in 10 high power fields.
0=no staining,
1+= distinct membrane staining visible at 40X magnification only
2+= distinct membrane staining visible at 10X magnification only
3+= distinct membrane staining visible at 5X magnification only.
Results
The results of immuno-histochemical analysis of all 11 patients,(Table 2) confirmed histopathologically as cholecystitis are given below:
ErbB-1 evaluation was positive in 7/11(63.64%) and negative in 4/11 (36.36%) patients [Figure.1,2,3]
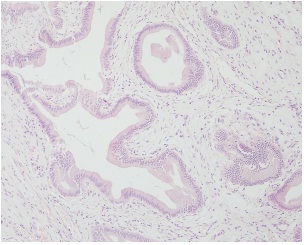
Figure 1: Chronic cholecystitis. H&E, 10X
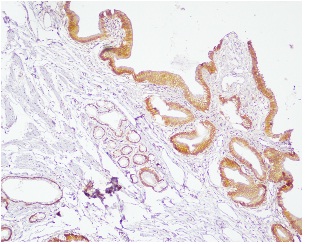
Figure 2: Chronic cholecystitis showing positive staining for EGFR (>90%, 3+). IHC, 10X
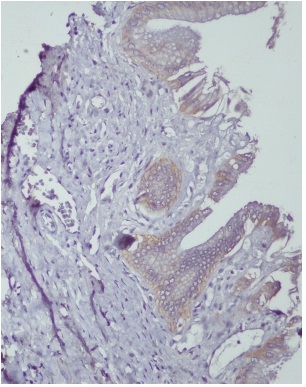
Figure 3: Chronic cholecystitis showing positive staining for Her 2 neu (60%, 1+). IHC, 20X
Authors like Lee CS et al (1995) [9] found 7/11 pts (64.00%) positivity in their study but few have negative results in 10 patients. In positive cases (n=7), subset of expression was 1+ in 5/7 (71.42%), 2+ in 1/7 (14.29%) and 3+ in 1/7 (14.29%). ErbB-2 was positive in 9/11(81.82%) and negative in 2/11 (18.18%) patients (Table 2).
29/46 patients (63.00%) as in our study [2] but Kamel D et al (1993) showed negative results in 4 patients (0%). In positive cases (n=9), subset of expression was 1+ in 1/9 (11.11%), 2+ in 5/9 (55.56%) and 3+ in 3/9 (33.33%).Other study have reported 2+ in (12.5%) patients [6].
As we have seen above, there are both positive and negative results are present in the literature. This was being a pilot study, the association between ErbB-1 and ErbB-2 is not found to be significant (p value=0.6351) but large numbers of pts., are required for better and consistent results in our setup.
BTC are uncommon in the United States but are endemic in South America and Asia. These are aggressive tumors associated with poor prognosis and survival. Standard chemotherapy often offers minimal benefit. Activation of ErbB-2 (HER-2/neu) and/or ErbB (EGFR) are important in breast, colon, lung cancer with exploration of its role in BTCs has been going on [6]. ErbB-2 (HER-2/neu) activates the Akt/NF-kappa B anti-apoptotic cascade to confer resistance to tumor necrosis factor (TNF) on cancer cells which ultimately reduce host defence against neoplasia [7].
ErbB (EGFR) mutations were more common in intra-hepatic or poorly differentiated tumors. Differences in age, sex, stage at diagnosis and survival was not observed between mutation positive and negative pts. Therefore, a highly selected application of the ErbB (EGFR) kinase inhibitor would be therapeutically effective in these patients [8].
Cholelithiasis and cholecystitis were closely related to GBC. The positive expression rates of epidermal growth factor (EGF) and epidermal growth factor receptor (EGFR) were higher in GBC and dysplasia than in simple hyperplasia and normal gallbladder tissue. Significant positive correlation was shown between EGF, EGFR and PCNA (proliferating cell nuclear antigen) [9].
There is increasing evidence that overexpression of tyrosine kinase growth factor receptors such as ErbB-2, EGFR and Met may play important roles in the development of BTC [10]. Lapatinib is an oral inhibitor of EGFR and Her2/neu with evidence of activity in a number of tumor types. In a case report, dramatic response has been quoted to Panitumumab and Bevacizumab in widespread metastatic GBC [11]. Further understanding of the molecular mechanism of carcinogenesis coupled with more extensive genetic profiling of GBC pts., will help to assess the therapeutic relevance of targeting a specific pathway [12].
Conclusions
Cholelithiasis and cholecystitis were closely related to GBC. We have to analyze the pathway by which these relations take place and check it in between. Although anatomically BTCs are related and have similar metastatic patterns, each has a distinct clinical presentation, molecular pathology and prognosis. Understanding the molecular events in gallbladder carcinogenesis may provide novel targeted therapeutic approach as well as prediction of getting cancer in cholecystectomy pts., needs further research in this regard. As this was a pilot study in our set up and sample size is small, we require more number of pts., for more appropriate and consistent results. ErbB-1 and ErbB-2 should be evaluated as predictive and prognostic marker in future studies.
Authors’ contribution
RH designed, coordinated and conducted the study, prepared
and revised the manuscript.
AS coordinated the study and helped in preparing
the manuscript.
SM coordinated and conducted the study.
NPA coordinated
the study and assisted in preparing the manuscript.
Ethical Considerations
The study was approved by the Institute Ethics committee. Written informed consent was taken from all the participating patients
Conflict of Interests
As an author of the article along with all my co-authors, I disclose that there is no conflict of interest. I, hereby also disclose that this article has not been submitted to any other journal nor this is under review or in the process of publication.
Funding
None Declared
Acknowledgement
None
References
[1].Sergeant G, Lerut E, Ectors N, Hendrickx T, Aerts R, Topal B. The prognostic relevance of tumor hypoxia markers in resected carcinoma of the gallbladder. Eur J Surg Oncol. 2011; 37: 80-6.[Pubmed]
[2].Chow NH, Huang SM, Chan SH, Mo LR, Hwang MH, Su WC. Significance of c-erbB-2 expression in normal and neoplastic epithelium of biliary tract. Anticancer Res. 1995; 15: 1055-9[Pubmed]
[3].Kaufman M, Mehrotra B, Limaye S et al. EGFR Expression in Gallbladder Carcinoma in North America. Int J Med Sci 2008; 5: 285-291.[Pubmed]
[4].Ooi A, Suzuki S, Nakazawa K et al. Gene amplification of Myc and its Coamplification with ERBB2 and EGFR in gallbladder adenocarcinoma. Anticancer Res.2009; 29: 19-26.[Pubmed]
[5].Chaube A, Tewari M, Garbyal RS, Singh U, Shukla HS. Preliminary study of p53 and c-erbB-2 expression in gallbladder cancer in Indian patients’ manuscript id: 8962091628764582. BMC Cancer.2006; 10: 126.[Pubmed]
[6].Kawamoto T, Krishnamurthy S, Tarco E et al. HER Receptor Family: Novel Candidate for Targeted Therapy for Gallbladder and Extrahepatic Bile Duct Cancer. Gastrointest Cancer Res. 2007; 1: 221-7.[Pubmed]
[7].Zhou BP, Hu MC, Miller SA et al. HER-2/neu blocks tumor necrosis factor- induced apoptosis via the Akt/NF-kappa B pathway. J Biol Chem. 2000; 275: 8027-31.[Pubmed]
[8].Gwak GY, Yoon JH, Shin CM et al.(2005) Detection of response predicting mutations in the kinase domain of the epidermal growth factor receptor gene in cholangiocarcinomas. Journal of Cancer Research and clinical Oncology 131; 10: 649-652.[Pubmed]
[9].Zhou YM, Li YM, Cao N, Feng Y, Zeng F. Significance of expression of epidermal growth factor (EGF) and its receptor (EGFR) in chronic cholecystitis and gallbladder carcinoma. Ai Zheng. 2003; 22: 262-5.[Pubmed]
[10].Elizabeth Riley, Harry Carloss. Dramatic Response to Panitumumab and Bevacizumab in Metastatic Gallbladder Carcinoma. Oncologist 2011; 16: e1-e2.[Pubmed]
[11].Elizabeth Riley, Harry Carloss. Dramatic Response to Panitumumab and Bevacizumab in Metastatic Gallbladder Carcinoma. Oncologist 2011; 16: e1-e2[Pubmed]
[12].Zhu AX, Hong TS, Hezel AF, Kooby DA. Current Management of Gallbladder Carcinoma. The Oncologist. 2010 ;15: 168-18[Pubmed]


