Case Report

Anaplastic Variant of Diffuse Large B Cell Lymphoma (DLBCL) – A Rare and Dilemmatic Entity
1,Mona Bargotya, 2Kiran Agarwal, 3Shailaja Shukla
- 1Department of Pathology, Lady Hardinge Medical College, New Delhi
- Submitted Sunday, June 08, 2014
- Accepted:Friday, July 25, 2014
- Published Sunday, August 03, 2014
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Background
Anaplastic variant of DLBCL is a morphological variant of DLBCL (NOS) characterized by presence of large to very large round, oval or polygonal cells with bizarre pleomorphic nuclei that may resemble Reed –Sternberg cells and tumor cells of anaplastic large cell lymphoma(ALCL), thereby rendering them diagnostically challenging.
Case Report
A 36 year old male presented with rapidly growing swelling measuring about 10x8cm in upper lateral half of left pectoral region extending upto axilla, associated with fever and pain radiating to left arm since one month. Clinical diagnosis was suggestive of soft tissue sarcoma. CT scan revealed a large heterogeneously enhancing soft tissue mass in left axilla and anterolateral chest wall with internal necrotic areas and encasement of blood vessls . Fine needle aspiration cytology as well as excisional biopsy from left pectoral mass was done and revealed similar cytomorphological features. There was presence of large round, oval to polygonal bizarre cells with moderate amount of eosinophilic cytoplasm, marked nuclear pleomorphism and irregular nuclear membrane. Many of these cells showed embryoid nucleus and wreath like arrangement of nuclei. The presence of these neoplastic cells posed a morphological dilemma. However, immunohistochemistry turned out to be of utmost utility and helped to make the correct diagnosis of Anaplastic variant of DLBCL.
Conclusion
Because of high degree of nuclear anaplasia posing diagnostic difficulties, accurate clinical approach, morphological assessment and immunohistochemical correlation is the precise and recommended method to achieve the correct diagnosis.
Key Words
Anaplastic large cell lymphoma, Diffuse large cell lymphoma
Introduction
established in 2008, Anaplastic large cell lymphoma with immunophenotype B (ALCL-B) is a distinct morphological variant of the Diffuse large B cell lymphoma (DLBCL) [1] which was recognized by its expression of Ki-1 antibody, now CD30. Neoplastic cells that expressed CD30 derived from T-cells and they were denominated Ki-1 Lymphomas. However, it is now recognized that there is a small number of cases with the B immunophenotype [2]. This type of lymphoma appears in lymph nodes and is quite identical to its counterpart T-cell lymphoma. Anaplastic variant of DLBCL is a rare morphological variant of DLBCL (NOS) characterized by presence of large to very large round, oval or polygonal cells with bizarre pleomorphic nuclei that may resemble Reed –Sternberg cells and tumor cells of anaplastic large cell lymphoma (ALCL), thereby rendering them diagnostically challenging [1 3 4]. Herein, we are presenting a case of Anaplastic variant of DLBCL which posed a morphological diagnostic dilemma.
Case Report
A 36 years old male presented with rapidly growing swelling left side of chest extending upto axilla, associated with pain and fever since one month. On examination an ill defined, firm-hard swelling measuring 10x8cms in upper lateral half of left pectoral region extending upto axilla without any associated lymphadenopathy was noted. On this basis a clinical diagnosis of soft tissue sarcoma was made. CT scan revealed large heterogenously enhancing soft tissue mass in left axillary and anterolateral chest wall measuring 10x9x7cm with encasement of major vessels and internal necrotic areas. Clinical correlation was suggested. Fine needle aspitation cytology and imprint cytology was performed from the chest swelling showed similar features. The smears were cellular showing single cells and poorly cohesive groups of large anaplastic cells with moderate amount of cytoplasm and large pleomorphic vescicular nuclei. Many binucleate and multinucleate tumor cells with presence of doughnut, embryoid, reniform with occasional wreath cells were seen (Figure. 1). Based on these cytomorphological features, a diagnosis of Anaplastic large cell lymphoma was considered. Biopsy of the left pectoral mass revealed a partly encapsulated lymph node with thickened capsule, effacement of lymph node architecture and replacement by tumor cells showing a characteristic sinusoidal growth pattern. The tumor cells were large round oval bizarre with scant to moderate amount of eosinophilic cytoplasm with marked nuclear pleomorphism, irregular nuclear membrane, coarsely clumped chromatin (Figure. 2). Many binucleate and multincleate cells were seen. Many cells showing embryoid nucleus and wreath like arrangement of nuclei were also seen. On this morphological basis a differential diagnosis of ALCL, anaplastic variant od DLBCL and Hodgkin’s lymphoma was kept. Immunohistochemical panel for CD45, CD30, CD20, EMA, ALK, CD15 and CD5 was put. The present case showed strong positivity for CD20 and CD45, focal positivity for CD30 and EMA especially in the large anaplastic cells but however, was negative for ALK, CD15 and CD5 (Figure. 3)
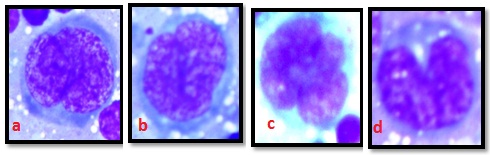
Figure 1: Different cytomorphological forms of tumor cells-(A) Embyroid cell (B) Doughnut cell (C) Wreath cell (D) Reniform cell (Giemsa x1000)
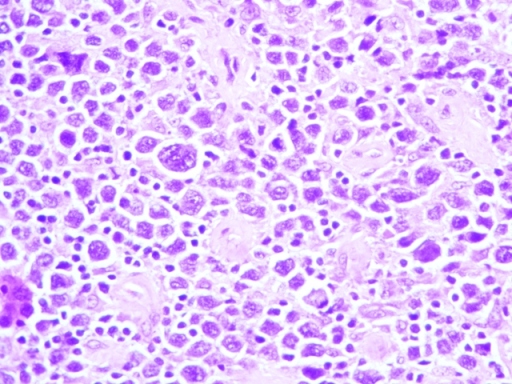
Figure 2:Large round oval bizarre tumor cells with scant to moderate amount of eosinophilic cytoplasm with marked nuclear pleomorphism, irregular nuclear membrane, coarsely clumped chromatin showing characteristic sinusoidal growth pattern.(H & E x400)
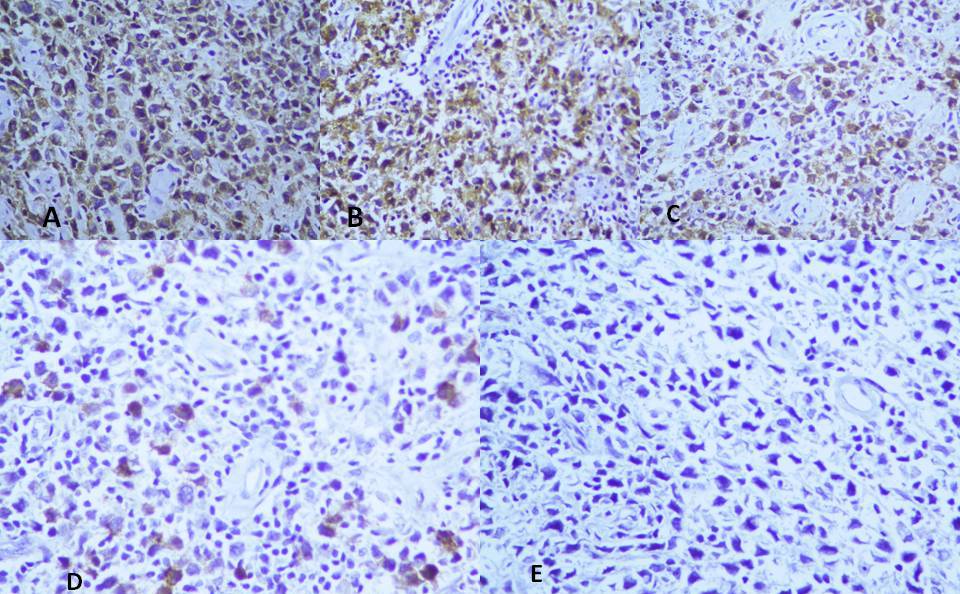
Figure 3: Tumor cells showing strong positivity for (A) CD45 (B) CD20 ; focal positivity for (C) CD 30 (D) EMA ; and negative for (E) ALK.
On the basis of these histopathological features as well as immunohistochemistry findings a final diagnosis of Anaplastic variant of DLBCL was made. The patient was immediately put on chemotherapy and the clinical course has been uneventful till date.
Discussion
The anaplastic variant of DLBCL is a rare morphological variant characterized by the presence of anaplastic, bizarre cells that may be arranged in a sinusoidal and/ or cohesive growth pattern. It is important to recognize this variant because of its propensity to mimic other lymphomas, particularly anaplastic large cell lymphoma [3 4]. Some of the tumor cells may also show a striking resemblance to Reed-Sternberg cells. There are few cases published of this entity and its frequency remains unknown. However, in the study performed by Weisenburger and colleagues, it represented 3.4% of total Non-Hodgkin lymphomas [5].The mean age of presentation being 57 years i.e older age group and male to female ratio of 1:1 [6] .
The morphological dilemma imposed by this entity can be excluded by the appropriate immunohistochemical studies [1]. Anaplastic variant of DLBCL and ALCL, though share many histological features, including very large cells with markedly pleomorphic nuclei, a sinusoidal growth pattern and CD30 positivity, they can be distinguished by virtue of B-cell lineage i.e. strong positivity for CD20, uniform CD45 expression, infrequent EMA positivity and the absence of ALK expression which characterizes Anaplastic variant of DLBCL. Because some of the cases of DLBCL may also be ALK positive, immunostains for ALK protein expression, as well as cytogenetic and molecular genetic study, should be incorporated in the analysis. The most commonly observed cytogenetic abnormality in ALK positive DLBCL is t(2;17)(p23;q23) or clathrin/ALK (7) while, the classic ALCL-related cytogenetic abnormality described is t(2;5)(p23;q35) or nucleophosmin/ALK [8]. They seem to have a poor prognosis and an aggressive course than DLBCL as well as ALCL [9 10]. Although the biologic nature of these neoplasms is yet to be defined, EBV may play a role in the pathogenesis of some of these neoplasms [11].
Conclusion
There are only few cases of this entity published and hence its frequency remains unknown. It closely mimics ALCL and is a diagnostic dilemma due to presence of similar morphology. Despite the morphologic and immunophenotypic similarities, anaplastic variant of DLBCL can be distinguished from ALCL by virtue of their B-cell lineage and lack of ALK expression. Prompt pathological diagnosis and initiation of chemotherapy are crucial to patient outcome. The recognition of ALK-positive DLBCL as a distinct entity is important because most patients follow an aggressive disease course and are unlikely to respond favorably to the current standard treatment protocol. It is important to consider the description of this variant in order to better understand its biology and morphological aspect for further studies.
Key Message
There are only few cases of this entity published and its frequency remains unknown. The aim is to present the clinical, morphological, and immunophenotypic characteristics of this variant exhibiting bizarre cellular morphology and thereby resembling ALCL.
Ethical Considerations
Written informed consent was obtained from the patient for publishing this case report.
Conflict of Interests
None
Authors’ Contributions
MB: Literature search and drafting of manuscript.KA: Histopathological diagnosis and edited final manuscript.SS: Cytological diagnosis
Funding
None
Acknowledgement
None
References
[1].Stein H, Warnke RA, Chan WC, Jaffe ES, Chan JKC, Gatter KC and Campo E. Diffuse Large B-Cell Lymphoma, Not otherwise Specified, In: Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, Vardiman JW, Eds., WHO Classification of Tumors of Haematopoietic and Lympoid Tissues, 4th Edition, WHO Press, Lyon .2008: 233-237.
[2].Lennert K, Feller AC. Histopathology of Non-Hodgkin’s Lymphomas based on the Updated-Kiel Classification, 2nd Edition, Springer-Verlag, Berlin. 1992:152.
[3].Haralambieva E, Pulford KA, Lamant L, et al. Anaplastic large cell lymphomas of B-cell phenotype are anaplastic lymphoma kinase (ALK) negative and belong to the spectrum of diffuse large B-cell lymphomas. Br J Haematol. 2000; 109: 584-591 [Pubmed]
[4].Lai R, Mederios LJ, Dabbagh L, Formenti KS, Coupland RW. Sinusoidal CD30 –positive large B-cell lymphoma: a morphologic mimic of anaplastic large cell lymphoma. Mod Pathol. 2000; 13: 223-228.[Pubmed]
[5].Weisenburger DD, Anderson JR, Diebold J, Gascoyne RD, Maclennan KA, Muller-Hermelink HK, Nathwani BN, Ullrich F, Armitage JO. Systemic Anaplastic large –Cell Lymphoma: results from the Non-Hodgkin’s Lymphoma Classification Project. American Journal of Hematology. 2001; 67(3):172-178 [Pubmed]
[6].Warnke RA, Weiss LM, Chan JKC, Cleary ML, Dorfman RF. Malignant lymphoma, diffuse, large cell and variants. In :Roai J, editor. Atlas of Tumor pathology: tumors of the lymph nodes and spleen. Washington, DC: Armed Forces Institute of Pathology .1994:153-220.
[7].Momose S, Tamaru J, Kishi H, Mikata I, Mori M, Toyozumi Y, Itoyama S. Hyperactivated STAT3 in ALK-positive diffuse large B-cell lymphoma with clathrin-ALK fusion. Hum Pathol. 2009;40:75–82.[Pubmed]
[8].Delsol G, Lamant L, Mariamé B, Pulford K, Dastugue N, Brousset P, Rigal-Huguet F, al Saati T, Cerretti DP, Morris SW, Mason DY. A new subtype of large B-cell lymphoma expressing the ALK kinase and lacking the 2; 5 translocation. Blood. 1997; 89(5):1483-90[Pubmed]
[9].Noordyun LA, Bruin PC, van Heerde P, van de Sandt MM, Ossenkoppele GJ, Meijer CJLM. Relation of CD 30 expression to survival and morphology in large cell B cell lymphoma. J Clin Pathol 1994; 47:33[Pubmed]
[10].Laurent C, Catherine Do, Gascoyne R D, Lamant L, Ysebaert L, Laurent G, Delsol G, Brousset P. Anaplastic Lymphoma Kinase–Positive Diffuse Large B-Cell Lymphoma: A Rare Clinicopathologic Entity With Poor Prognosis. Journal of Clinical Oncology. 2009; 27(5): 4211-16[Pubmed]
[11].Shimakage M, Nakamine H, Tamura S, Takenaka T, Yutsudo M, Hakura A. Detection of Epstein-Barr virus transcripts in anaplastic large-cell lymphomas by mRNA in situ hybridization. Hum Pathol 1997; 28:1415-9. [Pubmed]


