Case Report

Pneumo-cholecystitis in a jaundiced patient presenting with pneumoperitoneum
1Satyendra Kumar Tiwary, 1Ajay Kumar Khanna
- 1Department of General Surgery Institute of Medical Sciences, Banaras Hindu University, Varanasi – 221005
- Submitted: September 20, 2012
- Accepted: October 15, 2012
- Published: October 18, 2012
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background
Pneumo-cholecystitis is a rare disorder comprising approximately 1% of cases of acute cholecystits. Impaired vascularity with superimposed gas forming bacterial infections leads to pneumo-cholecystitis. Advanced age, diabetes mellitus, impaired immunity, atherosclerosis are predisposing factors.
Case Presentation
We managed a case of pneumo-cholecystitis in a jaundiced patient with hepatitis B infection, who presented with pneumoperitoneum. A thirty five year female had pain abdomen localized to right upper quadrant of abdomen for four days. Vague and tender lump (4cm x 7cm) below right subcostal margin and just lateral to rectus muscle was found on examination. Lab investigations revealed hepatitis B infection with deranged liver functions. Plain X-ray abdomen in revealed free gas shadow under diaphragm. USG revealed distended gallbladder but CT scan showed free gas in peritoneal cavity with distended gallbladder and gas in gallbladder lumen, wall and pericholecystic region settling the final diagnosis of pneumo-cholecystitis. She was clinically stable and no signs of peritonitis were present. Although treatment of choice for pneumo-cholecystitis is splenectomy we postponed surgery due to deranged liver function tests and hepatitis B infection and conservative treatment was used. Patient was discharged after one week and doing well during a follow up of 11 months.
Conclusion
Spontaneous pneumoperitoneum is an extremely rare finding in pneumo-cholecystitis. It should be ascertained that no visceral perforation is present, before proceeding for conservative management.
Key Words
Cholecystitis, gallbladder, free gas, bacterial infection, emphysematous cholecystitis.
Background
Pneumo-cholecystitis or emphysematous cholecystitis was first described by Stolz in 1901 during autopsy [1]. Lobinger reported intra-operative finding of gas in the gallbladder wall and lumen during surgery in 1908 [2]. Hegner first diagnosed this condition preoperatively using roentgenograms in 1931 [3]. Gangrene of gallbladder occurs in up to 74% of emphysematous cholecystitis patients. The average mortality rate associated with emphysematous cholecystitis is 15%, while that associated with acute cholecystitis is 4% [4]. Classical presentation is radiological evidence of gas in gallbladder fossa, lumen or peri-cholecystitic area. Abdominal CT scan is confirmatory for the presence of gas. Spontaneous penumoperitoneum, a finding typically associated with a ruptured viscus has been reported as an uncommon presentation of emphysematous cholecystitis [5,6].
Case Presentation
A thirty five year female presented with acute pain abdomen localized to right upper quadrant of abdomen for 4 days. Associated nausea and occasional vomiting was present. On Physical examination, she was deeply jaundiced with vague abdominal lump 4cm x 7cm below right subcostal margin and just lateral to rectus muscle. Tenderness was localized over the lump & other quadrants of abdomen were non-tender & soft on palpation.
Laboratory investigations revealed the patient to be infected with hepatitis B and deranged liver function tests (Total bilirubin 12.06 mg/dl; SGPT 661 IU/L; SGOT 552 IU/L; Alkaline phosphatase 1220 IU/L). Total leukocyte count was 21.6×109 /L with neutrophils 92%. Plain X-ray abdomen in erect posture revealed free gas shadow under diaphragm. Ultrasound of abdomen was not of much help as distended gallbladder was only finding. Abdominal CT scan showed free gas in peritoneal cavity with distended gallbladder and gas in gallbladder lumen, wall and pericholecystic region settling the final diagnosis of pneumo-cholecystitis (Figure 1).
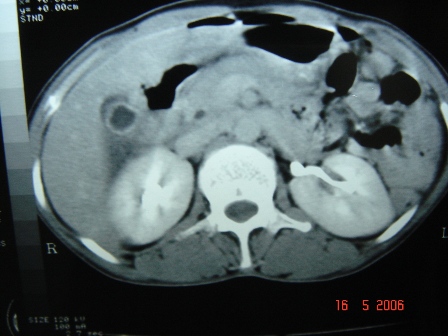
Figure 1.CT scan of abdomen showing gas in gallbladder lumen, wall and pericholecystic region.
Treatment of choice is surgical intervention and cholecystectomy. Our patient was stable clinically and no signs of peritonitis were present, so we decided to conserve the patient on intra-venous fluid support and empirical antibiotic therapy. Deranged liver function tests and hepatitis B infection were also considered for postponing surgery. After 72 hours, patient was allowed oral intake of liquids. Total leukocyte counts were decreased to 12.1 x 109/L with neutrophils 80%. Patient was discharged after one week. Liver function tests revealed improvement and patient was referred to department of gastroenterology for management of hepatitis B. She was doing well during a follow up of 11 months.
Discussion
Spontaneous pneumoperitoneum is an extremely rate presentation of emphysematous cholecystitis [5,6]. Pathogenesis is attributed to peri-cholecystic gas forming bacterial infection. Ultrasound has become one of the mainstays in the diagnosis of pathologic conditions of gallbladder. In emphysematous cholecystitis, ultrasound is difficult to interpret due to pericholecystic gas and absence of gall stones in majority of the cases [7]. Some times effervescent gallbladder may found on USG examination contributing to the diagnosis of emphysematous cholecystitis. Some times effervescent gallbladder may be found on USG examination contributing to the diagnosis of emphysematous cholecystitis [8,9]. Curvilinear gaseous artifacts in the gallbladder, the “ring-down effect” & “comet tail” are diagnostic of emphysematous choleystitis, but the frequency of these signs are unclear. CT scan demonstrates emphysematous changes in gallbladder wall that are diagnostic of this condition [9].
Earliest antibiotic administration with coverage against clostridia, streptococci and enterobacter should be the first line of management followed by surgical intervention in the form of open cholecystectomy. We initiated antibiotic therapy in our patient but postponed surgery due to active hepatitis B infection and deranged liver functions. Patient should be monitored carefully and closely to detect complications e.g. perforation, sepsis, peritonitis.
Conclusion
Spontaneous pneumoperitoneum is an extremely rare finding in pneumo cholecystitis. Treatment of choice for pneumo cholecystitis is cholecystectomy but it can be managed by conservative treatment and follow up if no visceral perforation is present.
Author's Contribution
SKT: Literature search and preparation of draft manuscript.
AKK: Editing of the final manuscript.
Both authors have read the manuscript and approved the manuscript for publication in WJSR.
Conflict of Interest
The authors declare that there are no conflict of interests
Ethical Considerations
Written informed consent was obtained from the patient for publication of this case report. The copy of the consent is available with authors.
Funding
None
Reference
[1]. Stolz A. Uber gasbildung in den Gallenwegen. Virchow Arch Pathol Anat. 1901; 165: 90-123.
[2]. Lobinger AS. Gangrene of the gall bladder. Ann Surg. 1908; 48: 72 - 9.[Pubmed]
[3]. Hegner CF. Gaseous pericholecystitis with cholecystitis and cholelithiasis. Ann Surg. 1931; 22: 993 - 1000.
[4]. Mentzer RM, Golden GT, Chandler JG, et al. A comparative appraisal of emphysematous cholecystitis. Am J Surg. 1975; 129: 10-15.[Pubmed]
[5]. Watson DI, Isaacs J, Williams RS. Emphysematous cholecystitis can cause pneumoperitoneum. Aust N Z J Surg. 1994; 64: 130-31.[Pubmed]
[6]. Radin DR, Halls JM. Emphysematous cholecystitis presenting with pneumoperitoneum. AJR. 1987; 149: 1175- 6.[Pubmed]
[7]. Yeatman TJ. Emphysematous cholecystitis: an insidious variant of acute cholecystitis. Am J Emerg Med. 1986; 4: 163-6.[Pubmed]
[8]. Nemcek AA Jr, Gore Rm, Vogelzang RL, et al. The effervescent gallbladder: a sonographic sign of emphysematous cholecystitis. AJR. 1988; 150:575-7.[Pubmed]
[9]. Gill KS, Chapman AH, Weston MJ. The changing face of emphysematous cholecystitis. Br J Radiol. 1997; 70:986-91.[Pubmed]

