Letter to Editor

Mesenteric cyst – laparoscopic excision
1Sujit K Prasad, 1Ravindra Patel, 2Anuj K Srivastava
- 1Consultant Surgeon, MGM Hospitals, Navi Mumbai 400706, India
- 2Department of surgery, additional professor, SSR Medical College, Mauritius
- Submitted: November 12, 2012
- Accepted: December 28, 2012
- Published: January 12, 2013
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Mesenteric cyst is a rather uncommon disease. It is classified into four types namely chylolymphatic, enterogenous, urogenital remnant and dermoid (teratomatous). They may be asymptomatic or may present with recurrent abdominal pain or even as an acute abdomen. Laparoscopic management of this condition is feasible and rewarding.
Key words
Mesenteric cyst, chylolymphatic, excision, laparoscopic.
Introduction
Mesenteric cyst was first reported in 1507 and only 820 cases have been reported so far [1-4]. We present a case chylolymphatic mesenteric cyst managed laparoscopically.
A 61 year old patient had the presenting symptoms of diffuse intermittent colicky pain in the abdomen of varying magnitude for several years.
On clinical examination there was fullness and mild tenderness in the right half of abdomen.
USG findings
A well defined anechoic area in the right iliac fossa measuring 14 x 8 x 7 cm, displacing the bowel loops medially and abutting the lower pole of the right kidney. Hyperechoic areas are seen in the upper right lateral wall of the lesion.
CT findings
A well defined cystic mass in the right side of abdomen measuring 14 x 8 x 8 cm. It extends from the lower pole of right kidney to the right iliac fossa. It has thin partially calcified walls. No solid components. No septae. It touches the lower pole of right kidney and ileal loops. There is duplication of right upper ureter – they unite in the pelvis in front of the sacrum.
Operative findings and procedure
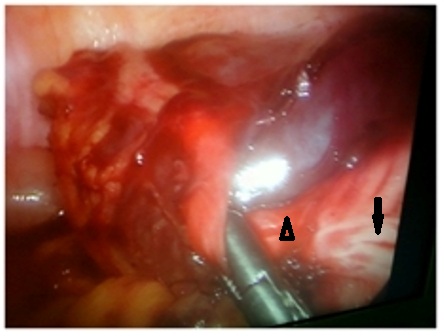
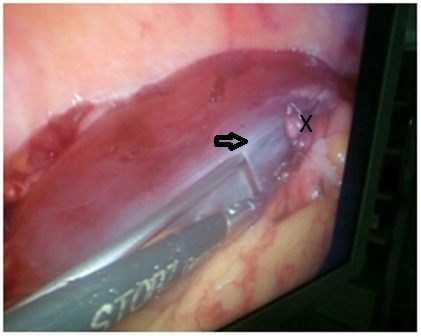
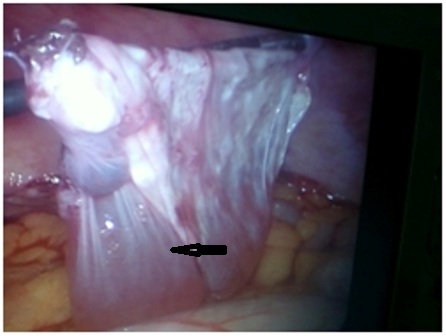
On initial laparoscopy, a large cyst was seen in the right paracolic gutter. The appendix, which appeared like a band of fibrous tissue, was plastered transversely across the cyst (Figure 1). As the appendix was dissected free and the stretch released, (Figure 2) the normal tubular shape became evident. A standard laparoscopic appendicectomy was done. The cyst was then carefully dissected free without puncturing it. The distension of the cyst was used to advantage in dissection. Finally the fluid was aspirated and the collapsed cyst removed (Figure 3 and 4).

Authors’ Contribution
SKP : Prepared the draft manuscriptRP: Did the literature search and prepared the draft manuscriptAKS: Final editing of the manuscript, concept and design.
Conflict of interests
The authors declare that there are no conflicts of interests.
Funding
None
References
[1]. Kuan E, Lau H, Yuen WK: Laparoscopic resection of mesenteric cyst. Gastrointestinal Endosc 2004, 59(1):154-156. [Pubmed].
[2]. Sahin DA, Akbulut G, Saykol V, San O, Toykol C, Dilek ON. Laparoscopic enucleation of mesenteric cyst: A case report. The Mount Sinai Journal of Med 2006, 73(7):1019-1020. [Pubmed].
[3]. Dequanter D, Lefebvre JC, Belva P, Takieddine M, Vaneuken P; Mesenteric cyst a case treated by laparoscopy and a review of literature. Surg Endosc 2002,16(10):1493. [Pubmed].
[4]. Shamiyeh A, Rieger R, Schrenk P, Wayand W; Role of laparoscopy in treatment of mesenteric cyst. Surg Endosc 1999, Sep;13(9):937-9. [Pubmed].

