Original Article

Giant Frontal Mucocele
*Vivek Shrama,Divye Prakash Tiwari and Deepak Patil
- *Department of NeurosurgeryInstitute of Medical Sciences,Varanasi-221005,India
- Saturday, October 05, 2013
- Thursday, October 17, 2013
- Friday, November 01, 2013
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction
Mucocele is a epithelium lined mucous containing sac that usually develops following blockage of ostium of paranasal sinuses.Giant frontal mucoceles are relatively rare and they may haveorbital, extra cranial and anterior cranial fossa extension
Material and methods
All cases of frontal mucoceles reported to neurosurgery in last 10 years were reviewed and only those having swelling at forehead were taken in our study. All such giant mucoceles were analysed in respect of size, bone involvement, age and symptoms.
Results
We are presenting a series of 17 cases of giant frontal mucoceles admitted over a period of 10 years in our university hospital highlighting the clinical features, radiological findings of this uncommon condition.
Conclusion
The frontal mucocele is common but its gaint variant is relatively not usually seen in modern era. The diagnosis is easy. The investigation of choice is CT scan with 3-D reconstruction. Treatment strategy is exentration of mucous membrane followed by bone cement cranioplasty.
Keywords
Giant frontal mucocele,Paranasal sinus mucocele,mucocel
Introduction
Mucocele is an epithelium lined mucous containing sac that usually develops following blockage of ostium of paranasal sinuses. Mucoceles of paranasal sinuses are most commonly seen in frontal sinus followed by ethmoidal sinus [1]. Mucoceles erode bone and invade adjoining intraorbital and intracranial cavity. Giant frontal mucoceles are rare [4,12] and they haveorbital, extra cranial and anterior cranial fossa extension [1,3]
Patients and Methods
All cases of frontal mucocele with obvious swelling on forehead reported to neurosurgery in last 10 years were taken into study. They were analysed in respect to age, sex, symtoms, radiology and management. Their incidence, aetiology and treatment protocol were discussed.
Observations
We have encountered 17 cases of gaint frontal mucocele with obvious swelling on the forehead. The maximum incidence (9 cases) were found in the age group 21-40 while 5 and 3 patients were belonged to age group of 0-20years 40 -60 years table 1.
| Age (years) |
Sex |
Incidence |
| 0-20 |
Male |
2 |
|
Female |
3 |
| 21-40 |
Male |
7 |
|
Female |
2 |
| 41-60 |
Male |
3 |
|
Female |
0 |
There is male predominance with ratio of 2.4 versus 1. Out of 4 patients with size 3 cm one presented with epilepsy, while the remaining presented with frontal headaches. One patient had bony involvement. All six patients with size 3-6 cm had frontal headache as their presenting symptom (Fig 1).

Figure 1: Giant frontal mucocle presenting as a large subcutaneous swelling
Diplopia and proptosis were seen in 2 patients whereas meningitis occurred in one patient (table 2).
| Supraorbital swelling size
(in cm)
|
Incidence |
Bony involvement
(Other than anterior wall)
|
Symptoms |
| <3cm |
4 |
1 |
Epilepsy (1),frontal headache(4) |
| 3-6 cm |
6 |
4 |
Frontal headache, diplopia (2), proptosis (2),meningitis(1) |
| >6 cm |
7 |
7 |
Asmptomatic except swelling(2),diplopia (2) Frontal headache(5), proptosis (2), meningitis(1) |
The four patients had bony involvement while two had complete destruction of the superior orbital wall. Two patients with swelling 6 cm was asymptomatic Fig 2.

Figure 2: Giant frontal mucocele in a 60 years male
Five patients (29.4%) presented with frontal headache, with 2 patient having proptosis and diplopia. One patient presented with meningitis. All 7 patients in this group had bony involvement with 4 patients having complete destruction of the superior orbital wall and one patient having posterior frontal sinus wall completely destroyed with the swelling directly abutting the dura.
Radiology
All patients were radiologically surveyed by plain skiagram and helical CT scan with 3D recontruction to define the limit of bony destruction ( Fig 3-6).

Figure 3: CT scan axial sectionof giant left frontal mucocele
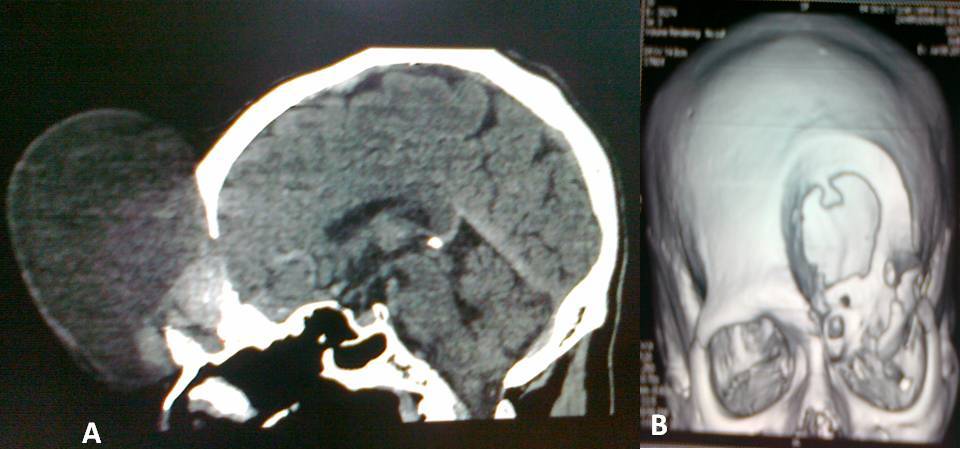
Figure 4: CT scan (a) sagittal section and (b) 3 D view renstruction showing bony defect of giant left frontal mucocele

Figure 5: sagittal section of frontal mucocele
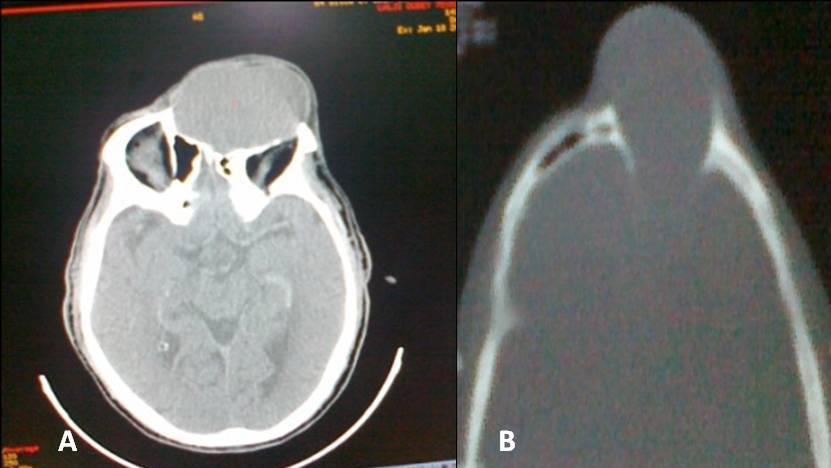
Figure 6. CT scan (a) axial cut brain and (b) bone window: a giant right frontal mucocele
Four patients had superior orbital margin involvement while the posterior boundary was lost in one.
Table 3. Computed Tomographic finding in gaint froantal mucocele
| Anatomical site |
Radiological Finding |
Number of cases |
Status of wall
1. Anteriorwall
2.Posterior wall
3.Orbital wall
|
Destroyed
Destroyed
Destroyed
|
17
6
8
|
| Attenuation value of content |
0-5
6-10
11-15
|
2
11
4
|
| Frontal Bone |
Size of defect of anterior wall in 3-D Less than 5cm
More than 5 cm
|
10
7
|
Treatment
All patients were operated upon through supraorbital orbital route followed by aspiration for bacterial analysis and exenteration of mucosal linning. The bony prominent edges were drilled out. The cranioplasty was done in 10 cases in second stage surgery while ten refused for cosmetic correction and accepted the mild depression. The recurrence was not observed in any case
Discussion
Frontal mucoceles are the most common (65%) amongthe paranasal sinus mucoceles [1].The continuous or intermittent obstruction of the sinus ostiumcauses dilatation of the sinus cavity secondary toaccumulation of mucoid material [2].Histopathology shows a hyperplastic mucosa withmetaplasia and peripheral fibrous reaction [14].Fibroblasts lining the mucoceleproduce interleukins and collagenase which leads to bone erosion [15,16]. Frontal mucoceles can present with adecreased visual acuity,visual field abnormalities, proptosis, ptosis, periorbitalswelling, displacement of the globe, restricted ocularmovements or as asymptomatic subcutaneous swelling [15,16]Frontal mucoceles tendto erode the thin bone of the superior orbital wall, invadingthe orbital cavity and displacing the globe inferiorly resultingin diplopia [18]. Direct compression of the optic nerve bythe mucoceleis rare so patient’s visual acuity is usually notaffected [18]. The mucocle can erode the posterior frontal sinus wall and invade into anterior cranial fossa. CT is the preferred mode of imaging for paranasal sinuspathologyas mucocle causes bony involvement [19].MRI is useful in complicated caseswith intracranial extension or infection. Sinus mucocele in CT is depicted as a non-enhancing,low attenuation expansile massusually isodense to brain, depending on the watercontent of the mucus. To the best of our knowledge, only three patients presenting withcomplaint of a frontal mucocele with intracranialextensionwith subcutaneous swelling have been reported so far [20,21].
Conclusion
The giant frontal mucocele is uncommon complication of sinusitis and usually affect middle aged male community.The presentation is obvious swelling, headache, proptosis. The diagnostic investigation is spiral computed scan. Surgery is ideal mode of treatment with excision and cranioplasty with almost no recurrence.
Conflict of interest
The authors declare that there are no conflicts of interest.
Authors' Contribution
VS: Concept and design of study, final approval
DPT: Analysis of cases, literature search and preparation of final manuscript
KS: Concept of study
DP: Addition of recent cases and prelimary preparation of
article
References
[1] Mokrim B, Touhami M, Chekkoury-Idrissi A, Benghalem A, Laraqui NZ,Kadiri F, Mellah N, Detsouli M, Benchakroun Y. Ethmoid-frontal mucocele.Apropos of 15 cases from 1985 to 1990. Rev Laryngol Otol Rhinol (Bord) 1991; 112(5): 429–431.[pubmed]
[2] Delfini R, Missori P, Iannetti G, Ciappetta P, Cantore G. Mucoceles of the paranasal sinuses with intracranial and intraorbital extension: report of 28 cases. Neurosurgery 1993; 32(6): 901–906.[pubmed]
[3] Weber R, Draf W, Keerl R, Constantinidis J. Aspects of frontal sinus surgery. III: Indications and results of osteoplastic frontal sinus operation. HNO 1995; 43(7): 414–420[pubmed]
[4]Lunardi P, Missori P, Di Lorenzo N, Fortuna A. Giant intracranial mucocele secondary to osteoma of the frontal sinuses: report of two cases and review ofthe literature. Surg Neurol 1993; 39(1): 46–48.[pubmed].
[5] Kawaguchi S, Sakaki T, Okuno S, Ida Y, Nishi N. Giant frontal mucocele extending into the anterior cranial fossa. J Clin Neurosci 2002; 9(1): 86–89.[pubmed].
[6] Chiarini L, Nocini PF, Bedogni A, Consolo U, Giannetti L, Merli GA. Intracranial spread of a giant frontal mucocele: case report. Br J Oral Maxillofac Surg 2000; 38(6): 637–640.[pubmed].
[7] Nakajima Y, Yoshimine T, Ogawa M, Takanashi M, Nakamuta K, Maruno M, Hasegawa H, Yokota J. A giant intracranial mucocele associated with an orbitoethmoidal osteoma. Case report. J Neurosurg 2000; 92(4): 697–701.[pubmed].
[8] Nakayama T, Mori K, Maeda M. Giant pyocele in the anterior intracranial fossa – case report. Neurol Med Chir (Tokyo) 1998; 38(8): 499–502.[pubmed]
[9] Van Manen SR, Bosch DA, Peeters FL, Troost D. Giant intracranial mucocele. Clin Neurol Neurosurg 1995; 97(2): 156–160.[pubmed]
[10] Hashim AS, Asakura T, Awa H, Yamashita K, Takasaki K, Yuhi F. Giant mucocele of paranasal sinuses. Surg Neurol 1985; 23(1): 69–74.[pubmed].
[11] Adekeye EO, Ord RA. Giant frontal sinus mucocoele. Report of two cases. J Maxillofac Surg 1984; 12(4): 184–187.[pubmed]
[12] Suri A, Mahapatra A K, Gaikwad S, Sarkar C. Giant mucoceles of the frontal sinus: a series and review. J Clin Neuroscience (2004) 11(2):214-215[pubmed].
[13] Fougeront B, Lamas G, Beltran M,Youssefi K, Soudant J. Frontal and ethmoidal mucoceles. Apropos of 17 cases. Ann Otolaryngol Chir Cervicofac 1990; 107: 323–327.[pubmed]
[14] Lund VJ, Milroy CM. Fronto-ethmoidal mucoceles: a histopathological analysis. J Laryngol Otol 1991; 105: 921–923[pubmed].
[15] Lund VJ, Henderson B, Song Y. Involvement of cytokines and vascular adhesion receptors in the pathology of fronto-ethmoidal mucoceles. Acta Otolaryngol Stockh 1993; 113: 540–546.[pubmed]
[16].Sharma GD, Doershuk CF, Stern RC. Erosion of the wall of the frontal sinus caused by mucopyocele in cystic fibrosis. J Pediatr 1994; 124: 745–747.[pubmed]
[17] Tan CS, Yong VK, Yip LW, Amritj S. An unusual presentation of a giant frontal sinus mucocele manifesting with a subcutaneous forehead mass. Ann Acad Med Singapore 2005;34:397-8.[pubmed]
[18] Tasman W, Jaeger EA. Duane’s Clinical Ophthalmology. Vol 2. NewYork: JB Lippincott Co, 1994:3-7.
[19].Rao VM, Sharma D, Madan A. Imaging of frontal sinus disease:concepts, interpretation, and technology. Otolaryngol Clin North Am 2001;34:23-39[pubmed]
[20] Akiyama M, Inamoto N, Hashigucci K. Frontal mucocele presenting as a subcutaneous tumour on the forehead. Dermatology 1999; 199:263-4.[pubmed]
[21]. Tan CSH , Yong VKY, Yip LW , Amrith S,An Unusual Presentation of a Giant Frontal Sinus Mucocele Manifesting with a Subcutaneous Forehead Mass. Ann Acad Med June 2005; 39(5):397-398[pubmed].
[22].Borkar S,Tripathi A K,Satyarthee G,Sharma B S,Mahapatra AK;Frontal Mucocele Presenting with Forehead Subcutaneous Mass: An Unusual PresentationTurkish Neurosurgery 2008, Vol: 18, No: 2, 200-203[pubmed]

