Case Report

Rare Presentation of Inguinal Hernia in Female: A Case Report
1Seema Khanna, 1Shashi Prakash, 1Seema Singh, 1S K Gupta
- 1Department of General Surgery, Institute of Medical Sciences, Banaras Hindu University, Varanasi (U.P.), India.221005
- Submitted: December 23, 2012;
- Accepted: January 11, 2013
- Published: January 17, 2013
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Inguinal hernia with uncommon contents in the hernia sac has been reported in the literature. Preoperative ultrasound can be helpful to diagnose the presence an uncommon content in the hernia sac. Here we report a rare case of adult female having inguinal hernia with sac containing atrophied uterus.
Keywords
Hernia, uncommon contents, atrophied uterus.
Introduction
Inguinal hernia is though less common in females as compared to males but is not an uncommon entity. The differential diagnosis of an inguinal mass includes hernia, mesothelial cyst, cystic lymphangioma, adenopathy, endometriosis, and varices [1,2]. Literature has revealed few uncommon contents in the hernia sac in females but to the best of our knowledge, there are only few reports of presence of uterus, fallopian tube and ovary in the female inguinal hernial sac. We here report an interesting and rare case of inguinal hernia in an adult female containing atrophied uterus in the hernia sac.
Case Report
25 year female presented with Reducible swelling in her left groin for 1 month. Patient was having primary amenorrhea. Local examination revealed a reducible swelling in her left inguinal region with positive cough impulse and deep ring occlusion test suggesting the indirect inguinal hernia.
Ultrasonography revealed- congenital atrophied uterus and left inguinal hernia.
Patient was operated with open approach, external oblique aponeurosis was opened and sac was dissected. Sac was found having atrophied uterus as its content which was then sacrificed and Lichenstein’s hernia repair was done (Figure 1).
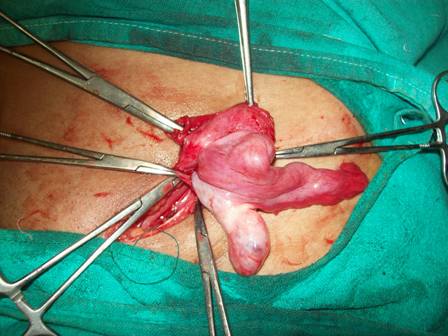
Figure 1- Atrophied uterus as the content of the hernia sac.
Histopathological examination confirmed of atrophied uterus.
Discussion
Obesity, pregnancy, and operative procedures have been shown to be risk factors that commonly contribute to the formation of inguinal hernia in females. However, to our knowledge, all of these risk factors have never been quantified. The reports of published case series of female inguinal hernia have emphasized the different, but favorable, stronger inguinal anatomy in females. Indeed, this explains the lower incidence in females, but it does not explain why some females do acquire an inguinal hernia.
Inguinal hernia may sometime surprise the surgeon with its unusual content [3,4] and hence may pose problems in surgical management. The hernia sac in inguinal hernia has been reported having almost all intra abdominal contents including stomach and their pathologies [5,6]. Acute conditions including perforated diverticular abscess have also been reported to track into the inguinal canal mimicking a strangulated inguinal hernia [7]. There is always a risk of significant extra-abdominal or intra-abdominal disease processes in patients with no evidence of bowel obstruction clinically and radiologically, presenting with painful inguinal swelling [7]. An infected hip prosthesis abscess, a subcutaneous fungal abscess, pancreatic psuedocyst [7], leaking abdominal aortic an-eurysms [8] and peritonitis have presented as an atypical inguinal hernia [9].
Entrapment of adenexae in an indirect inguinal hernia is rare in adult women. Most reported cases concern the pediatric population in whom ovaries and tubal herniation have long been associated as unusual contents [10]. The reported incidence of its occurrence is 71% in children under 5 years and 30% in adolescents or women in reproductive age group and 2.9% exclusively in adults [3]. At around 6 weeks of intrauterine life parietal peritoneum evaginates as processus vaginalis. The female counterpart of processus vaginalis usually disappears by 8 months of intrauterine life but may sometime persist as the canal of nuck. This persistence may be attributed to the hydrocele of the canal of nuck or inguinal hernia. Six girls having an infrequent condition, hydrocele of the canal of nuck, mimicking a sliding hernia with ovary has been reported previously. Hernia of the canal of nuck is also a rare condition and around 15-20% contain ovary, sometimes with a fallopian tube. Inguinal Hernia in two female infants containing uterus and uterine adenxa has also been reported [11]. Uterus as the content of hernia sac is still rarer and with thorough literature search, we have come across only a few cases of hernia in female infants containing uterus [12] but we have not come across any reported case in literature of hernia in an adult female containing atrophic uterus. Girls having uterine herniation cannot be well explained embryologically unless suspensory ligaments of the uterus possess any anatomical abnormality. One of the published reports laid the hypothesis that if there is failure of the fusion of the Mullerian ducts leading to the excessive mobility of the ovaries plus nonfusion of the uterine cornuae, the chance of herniation of the ovary into the inguinal canal is increased. Reports have documented of herniation of not only the ovary but fallopian tube and even the herniation of the entire uterus into the inguinal canal of female infants. Researchers have documented that when the ovary is herniated completely, only the fallopian tube is attached to the ligament in the sac and ovary and its vessels do not adhere to the sac itself. In cases when uterus also herniates, the herniated part of the uterus also adheres to the sac and needs a careful exploration. When the uterus found atrophied, as in our case, the only option remains is to sacrifice it along with repair of the hernia.
Conclusion
In females, hernia sac containing uterus, fallopian tube and ovary is very rare and is diagnosed by the characteristic sonographic appearance. It can be concluded that female patients of inguinal hernia should undergo ultrasound routinely so as to diagnose the rare contents of the sac.
Author’s Contribution
SP: Literature search and preparation of the main body of manuscript.
SS: Literature search and preparation of manuscript.
SK: Planning and execution of treatment and revision of the manuscript.
SKG: Final decision for the treatment and proof reading of manuscript before submission.
Conflicts of Interest
None
References
[1]. Chi C, Taylor A, Munjuluri N, Abdul-Kadir R. A diagnostic dilemma: round ligament varicosities in pregnancy. Acta Obstet Gynecol Scand 2005; 84:1126–1127. [Pubmed].
[2]. Oh SN, Jung SE, Rha SE, et al. Sonography of various cystic masses of the female groin. J Ultrasound Med 2007; 26:1735–1742. [Pubmed].
[3]. Gurer A, Ozdogan M, Ozlem N, Yildirim A, Kulacoglu H, Aydin R. Uncommon Content in Groin her-nia Sac. Hernia. 2006; 10: 152-5. [Pubmed].
[4]. Ballas K, Kontoulis T, Skouras Ch, Triantafyllou A, Symeonidis N, Pavlidis T, et al., Unusual Find-ings in Inguinal Hernia Surgery. Report of 6 Rare Cases. Hippokratia 2009;13: 169-171. [Pubmed].
[5]. Gibbons CE, Malhotra AK, Harvey MH. Inguinal Hernia an Unusual Case of Gastric Outlet Ob-struction. British Journal of Hospital Medicine 1994; 52: 360-361. [Pubmed].
[6]. Oruc MT, Kulah B, Saylam B, Moran M, Albayrak L, Coskun F. An Unusual Presentation of Metastatic Gastric Cancer Found during Inguinal Hernia Repair: Case Report and Review of Literature. Hernia 2002; 6: 88-90. [Pubmed].
[7]. Andrabi SI, Pitale A, El-Hakeem AA. Diverticular Abscess presenting as a Strangulated Inguinal Hernia: Case Report and Review of the Literature. Ul-ster Medical Journal 2007; 76: 107-108. [Pubmed].
[8]. Abulafi AM, Mee WM, Pardy BJ. Leaking Abdominal Aortic Aneurysm Presenting as an Inguinal Mass. European Journal of Vascular Surgery 1991; 5; 695-696. [Pubmed].
[9]. Sellu DP. Pus in Groin Hernia Sacs: A Complication of Non-Generalised Peritonitis. British Journal of Hos-pital Medicine 1987; 41: 759-760. [Pubmed].
[10]. Mayer V, Templeton FG. “Inguinal Ectopia of the Ovary and Fallopian Tube. Review of the Literature and Report of the Case of an Infant. Archives of Surgery. 1941; 43: 397-408.
[11]. Ming YC, Luo CC, Chao HC, Chu SM. Inguinal hernia containing uterus and uterine adenxa in female infants: Report of two cases. Pediatr Neonat 2011; 52:103-105. [Pubmed].
[12]. Kamio M, Nagata T, Yamasaki H, Yoshinaga M, Douchi T. inguinal hernia containing functioning, rudimentary uterine horn and endometriosis. Obstet Gynecol 2009;113: 563-566. [Pubmed].

