Case Report

Subserous Uterine Fibroid Presenting as Hemoperitoneum: A Case Report
1Somendra Pal Singh, 1Prashant Gupta, 2Manjaree Mishra ,1Anil Kumar Sharma, 1Shashi Prakash Mishra,
- 1Department of Surgery1 and Anesthesia2. UPRIMS&R, Saifai, Etawah (U.P.), India. 206130
- Submitted: Sunday, June 29, 2014
- Accepted: Tuesday, October 21, 2014
- Published:Sunday, November 09, 2014
This is an Open Access article distributed under the terms of the Creative Commons Attribution License ((http://creativecommons.org/licenses/by/3.0)which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Uterine fibroids are the most common of all the benign neoplasms affecting females in reproductive age groups. The subserous types of fibroids are rare in incidence but sometimes they present with rare complications as torsion of its pedicle or detachment from uterus resulting in a wandering variety of fibroid. Hemoperitoneum because of rupture of surface veins over these subserosal fibroids is very rarely encountered and reported. These patients usually present to emergency department with features of acute abdomen with hemorrhagic shock and need an urgent surgical intervention to take care of the problem.
Key words
Uterus, Fibroid, Subserous, Hemorrhage
Introduction
Uterine leiomyomais not an uncommon tumour of females in reproductive age groups but wandering or parasitic leiomyoma is rarely seen [1]. The most common complication parasitic uterine leiomyoma undergoesis torsion. Rarely do they present as acute abdomen due to hemoperitoneum because of bleeding from them. We are here presenting a case of bleeding from a uterine leiomyoma presenting with hemoperitoneum.
Case Report
A 45 years female presented to our surgical emergency department with history of acute onset severe pain abdomen and multiple episodes of vomiting for 8 hours. There was no history of abdominal trauma, drug intake or fever. Patient was perimenopausal without any past history of any kind of surgical intervention or any significant illness.
On examination patient was dehydrated, pale with cold and clammy skin. Pulse was very feeble and systolic blood pressure was 80 mm of Hg. Abdomen was distended and flanks were full. Tenderness was present over whole of the abdomen and board like rigidity was present. We made a provisional diagnosis of perforation peritonitis and after fluid resuscitation subjected patient for investigations. Hemoglobin was 6.5 gm/dl, X ray of chest and abdomen was normal. Ultrasonography of abdomen revealed presence of moderate to gross amount of free fluid inside peritoneal cavity which on diagnostic aspiration revealed frankly blood aspirate. There was also a complex mass present which was possibly arising from uterus and closely abutting bowel.
Packed cell transfusion was arranged and patient was shifted to operating room for emergency exploratory laparotomy.Patient was operated under general anesthesia with endotracheal intubation. On exploration there was around 1.5- 2 liters of blood present in peritoneal cavity and there was a huge mass with its pedicle attached to uterine fundus (Figure 1).
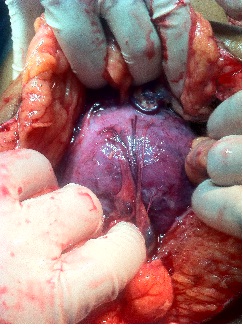
Figure 1: Showing fibroid on laparotomy
There was profuse bleeding from veins over the surface of massand mass was adhered with small bowel and sigmoid colon. Bleeding vessels were clamped; mass was carefully separated from surroundings; feeding vessels from surroundings were tied and cut; its pedicle was clamped, tied and mass was excised (Figure 2). Intraperitoneal drain was put and abdomen was closed. Patient received total 4 units of packed cell transfusion and her post operative course remained uneventful. Patient was well at discharge with Hemoglobin level 10 gm/dl. The Histopathological examination of the excised mass revealed features of a uterine leiomyoma.

Figure 2: Showing fibroid after its pedicle was clamped
Discussion
Uterine fibroids are the most common of all the benign neoplasms affecting females in reproductive age groups and may be intramural, subserosal, orsubmucosal in location [1]. Subserosal leiomyomasmay remain beneath the uterine surface or exophytic orpedunculated. Submucosal leiomyomas may sometimes protrudeinto the uterine cavity and may also becomepedunculated. If a pedunculated subserosal leiomyomadevelops an extremely long, tenuous stalk, it iscalled a wandering or migrating leiomyoma [2]. Such tumors may occasionally become adherent to surrounding structure as broad ligament oromentum and develop an auxiliary blood supply.The subserous type of fibroids are rare in incidence but sometimes they present with rare complications as torsion of its pedicle or detachment from uterus resulting in a wandering variety of fibroid [3]. Hemoperitoneum because of rupture of surface veins over these subserosal fibroids is very rarely encountered and rarely reported as well [4 5]. Authors have claimed few factors which may at times be responsible for bleeding from surface vessels of fibroid such as abdominal trauma, sudden exertion, straining and erosion of vessel by friction or pressure of the tumor against sacral promontory [5]. Congestion and excessive dilatation of the surface veins especially during menstruation, parturition, inflammation and torsion of the pedicle are possible factors for rupture of vessel on the tumor surface [2, 5, 6]. Other differential diagnosis for this case could be a ruptured ectopic pregnancy, ruptured ovarian cyst or torsion of adnexal tumours. Acute abdominal pain, tenderness, signs of hemorrhage together with presence of uterine fibroid may be highly suggestive of hemorrhage from ruptured surface vessels of fibroid [5 7]. Though our patient was having irregular menstrual cycles since past few months of this episode but has never consulted any gynecologist regarding her problems as she presumed the things occurring because she was approaching towards menopause. Patient was a housewife and she was routinely doing her household works which also included lifting water filled buckets from source of water supply few meters away from her home; which we think may have caused the problem. So we conclude that these kinds of patients usually present to emergency department with features of acute abdomen with hemorrhagic shock and need an urgent surgical interventionto take care of the problem [5 6 7 8] .
Authors’ Contribution
SPS: Concept and design, data acquisition and drafting of manuscript.
PG: Concept and design.
MM: data acquisition and drafting of manuscript.
AKS: Concept and design
SPM: Concept and design, data acquisition, and proof reading of final manuscript.
Conflict of Interests
The authors declare that there is no conflict of interests.
Ethical Considerations
Written informed consent was taken for publication of this case report.
Funding
None declared
Acknowledgement
None
References
[1].Lotterman S. Massive hemoperitoneum resulting from spontaneous rupture of uterine leiomyoma. Am J Emerg Med. 2008 Oct; 26(8):974.e1-2. doi: 10.1016/j.ajem.2008.02.029.
[Pubmed]
[2].Robbins SL, Cotran RS, Kumar V: Pathologic Basis of Disease. 3rd Ed. Philadelphia, WB Saunders, 1984, p 1109.
[3].Yeh HC, Kaplan M, Deligdisch L. Parasitic and Pedunculated Leiomyomas:Ultrasonographic Features. Journal of Ultrasound Med 1999; 18:789–794.
[Pubmed]
[4].Akahira J, Ito K, Nakamura R, Yajima A. Massive intraperitoneal hemorrhage and hypovolemic shock due to rupture of a coronary vessel of a uterine leiomyoma: a report of two cases. Tohoku J Exp Med. 1998; 185(3):217-22.
[5].Bangal V B*, Shinde K K, Gavhane S P, Ghorpade N, Gupta K and Gangapurwala S. Massive hemoperitoneum due to rupture of surface veins of a uterine leiomyoma. International Journal of Biomedical and Advance Research 2014; 05 (02):128-30.
[6].Dahan MH, Ahmadi R. Spontaneous subserosal venous ruptures overlying a uterine leiomyoma. A case report. J Reprod Med. 2002 May; 47(5):419-20.
[7].Sakhri J, Bakir D, Sabri Y, Ammara H. Hemoperitoneum secondary to the rupture of superficial veins of a uterine leiomyoma. Gynecol Obstet Fertil. 2002; (2):133-5.
[Pubmed]
[8].Horowitz E, Dekel A, Feldberg D, Rabinerson D. Massive hemoperitoneum due to rupture of an artery overlying a uterine leiomyoma: a case report. Acta Obstet Gynecol Scand 2005 Apr; 84(4):408-9.
[Pubmed]

