Original Article

Surgical ‘Hot Clinics’: What Do the Patients Think?
*Veeranna Shatkar, *Mohammad Imtiaz, *Mehmood Wain, *Thangadorai Amalesh
- *General surgery, BHR NHS Trust, Queens hospital, Romford, Essex, United Kingdom
- Submitted: Sunday, December 28, 2014
- Accepted: Friday, March 13, 2015
- Published: Sunday, March 22, 2015
This is an Open Access article distributed under the terms of the Creative Commons Attribution License ((http://creativecommons.org/licenses/by/3.0)which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Background
Surgical ‘hot clinics’ have been introduced recently in the UK and offer an alternate surgical care pathway with significant benefits to the NHS. The aim of this study was to explore the views of patients seen in surgical hot clinics.
Methods
All patients attending the surgical ‘hot clinic’ over a six-week period at a busy teaching Hospital in London, from Feb 2013 to March 2013 were included. The study was registered as an audit as it aimed to evaluate a new service. A questionnaire was specifically designed to explore patients’ experiences. No patient identifiable data was collected and patients were asked to complete the questionnaire after their consultation.
Results
115 patients attended the surgical ‘hot clinic’ over the study period. 58% of the patients were attending the clinic for the first time and the rest were follow-ups. 86% of the patients saw a nurse within 30 min of arrival. 79% saw a doctor within 60 minutes of arrival in clinic. Majority of the patients felt the clinical area was clean (98%). Majority of the patients felt that they were provided privacy (99%), involved in the decision-making (91%) and adequate information was provided (91%). Doctors and nurses were rated high (85%). 95% of patient rated their experience as 8 or above (scale of 10). Majority would prefer to be seen in the ‘Hot Clinics’ (83%) and would recommend it to family and friends (87%).
Conclusions
Surgical ‘Hot Clinic’ is an effective alternative surgical pathway, which is well received by patients.
Introduction
Emergency departments in the National Health Service (NHS, UK) are facing increased pressure in recent times due to increased emergency attendances. 24% of patients attending emergency department were admitted to hospital and 0.83 million acute beds were lost to delayed discharges in 2012-2013 in the UK (National Audit Office, UK). This not only has implications for patient care but also has obvious cost implications to the National Health Service (NHS). ‘Hot clinics’ have been introduced in various specialties, including surgery to provide quick access to specialist services to avoid delay and reduce the burden on the emergency department [1]. The Royal College of Surgeons has also acknowledged the sub-optimal delivery of emergency surgical care and laid out standards and guidance for delivery of unscheduled surgical care [2]. The introduction of these pathways may have an effect on patient care and experiences. The ‘high quality care for all’ report (2008) highlighted the importance of treating patients with compassion, dignity and respect in a safe and well-managed environment with patient experience at the heart of it (High quality care for all - NHS next stage review final report, 2008).
With these regulatory documents in mind, and to explore and improve patient care, this study was aimed to understand patient experiences of attending the surgical ‘Hot Clinic’.
Methods
This study was conducted by the Department of Surgery, Queen’s Hospital, Romford, UK over a 6-week period in Feb – Mar 2014. The surgical ‘Hot Clinic’ was started in our hospital with an aim to improve surgical emergency care and reduce the burden on the Emergency department. An audit done previously had shown huge benefits to the Department with the introduction of this service. We wanted to know patient experiences to evaluate and improve delivery of care by the ‘Hot Clinics’. As this study was a quality improvement process, ethical approval was not deemed necessary. The study was registered as an audit with the Audit Department, BHR NHS trust, London UK. A questionnaire was specifically designed to explore patient perspectives and experiences. All the patients were referred from General practitioners or from the surgical ward to the Surgical ‘Hot Clinics’. Patients were triaged by a nurse on arrival, and then seen by senior surgical doctor. Patients were then asked to fill in a questionnaire before leaving the clinic and to drop it in a box kept in the clinic. All data were anonymized and no patient identifiable data was used in this study.
Results
The questions and patient responses are summarized in (Table 1). Details of the surgical conditions are not addressed here as this paper only focuses on patient experiences.
|
How would you rate the standards of our waiting area?
|
|
Very good
|
Good
|
Average
|
Poor
|
Very poor
|
Don’t Know
|
|
60 (52.17)
|
53 (46.08)
|
2 (1.73)
|
0
|
0
|
0
|
|
How clean did you find the department?
|
|
Very clean
|
Fairly clean
|
Not very clean
|
Not at all clean
|
|
|
87(75.65)
|
25(21.73)
|
2(1.73)
|
1(0.86)
|
|
How long was the wait before seeing a nurse after booking in?
|
|
0-15 Min
|
16-30 Min
|
31-60 Min
|
> 60 Min
|
|
|
71 (61.73)
|
28 (24.34)
|
10 (8.69)
|
6 (5.21)
|
|
How long was the wait to see the Doctor?
|
|
0-30 Min
|
31-60 Min
|
61-120 Min
|
>120 Min
|
Do not know
|
|
|
70 (60.86)
|
21 (18.26)
|
16 (13.91)
|
4 (3.47)
|
4 (3.47)
|
|
Were you involved as much as you wanted in decisions about your care
and treatment?
|
|
All of the time
|
Most of the time
|
Some of the time
|
None of the time
|
Not applicable
|
|
|
90 (78.26)
|
15 (13.04)
|
6 (5.21)
|
1 (0.86)
|
3 (2.60)
|
|
Were you given enough privacy when you were seen in the clinic?
|
|
All of the time
|
Most of the time
|
Some of the time
|
None of the time
|
|
|
110 (95.65)
|
4 (3.47)
|
1 (0.86)
|
0
|
|
How do you rate the Doctors in the clinic?
|
|
Very good
|
Good
|
Fair
|
Poor
|
Very poor
|
No Answer
|
|
79 (68.69)
|
16 (13.91)
|
11(9.56)
|
1(0.86)
|
1(0.86)
|
7(6.08)
|
|
How do you rate the nurses in the clinic?
|
|
Very good
|
Good
|
Fair
|
Poor
|
Very poor
|
No Answer
|
|
79(68.69)
|
18(15.65)
|
0
|
0
|
0
|
18(15.65)
|
|
Do you feel you had enough information regarding your test results
and diagnosis?
|
|
Yes
|
More info needed
|
No
|
Not applicable
|
Don’t know
|
No answer
|
|
96(83.47)
|
8(6.95)
|
2(1.73)
|
5(4.34)
|
2(1.73)
|
2(1.73)
|
|
How likely are you to recommend our ‘Hot Clinic’ to family and
friends?
|
|
Extremely likely
|
Likely
|
Neither
|
Don’t know
|
No Answer
|
|
|
86 (74.78)
|
14 (12.17)
|
7 (6.08)
|
4 (3.47)
|
4 (3.47)
|
|
Would you prefer to be seen in the ‘Hot Clinic’ if needed for
similar problems in the future?
|
|
‘Hot Clinic’
|
Emergency Department
|
No Answer
|
|
|
95(82.60)
|
2(1.73)
|
18(15.65)
|
115 questionnaires were analyzed for this study. 60% patients were male and the rest were female. The mean age of patients was 45 (range: 16-85). 58% of patients were first time attenders referred directly by general practitioners with suspected acute surgical problems and the rest were follow-ups from the wards (patients who were discharged home from surgical wards) and hot clinic
98.25% of patients rated the waiting are as ‘very good’ or ‘good’, with the rest rating it as average. 97.38% felt that the clinical area was fairly or very clean. Majority of the patients (86.07%) saw a nurse with 30 minutes of booking of which 71% were seen with in 15 minutes of booking. 79.12% of patients said that a doctor saw them within 60 minutes of arrival in the ‘Hot Clinic’, of which 77% were seen within 30 minutes. 90.42% patients felt that they had adequate information given to them regarding the diagnosis and future management. 91.3% patients felt that they were involved in the decision making process of their treatment. 99.12% patients were happy that sufficient privacy was provided during the consultation in the ‘Hot Clinic’. 82.6% patients rated the doctors as good or very good. 84.34% of patients felt that the nurses were good or very good in the ‘Hot Clinic’. Two-third of the patients rated their overall visit experience 10 out of 10, 95 patients rated their experience as 8 and above (Figure 1). 95% patients preferred to be seen in the ‘Hot Clinic’ rather than the Emergency Department. 92% of patient would recommend the Surgical ‘Hot Clinic’ to their family and friends. Few patients made additional comments on their overall experience and were very pleased and thankful for the staff and the clinic environment.
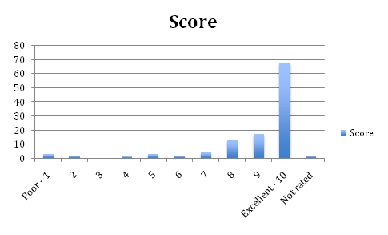
Figure 1: Figure showing the overall patient reported rating of the Surgical ‘Hot Clinic’ (Scale: 1=Poor to 10= Excellent)
Discussion
This study to our knowledge is a first of its kind to evaluate patient experiences in an alternate surgical emergency care pathway called Surgical ‘Hot Clinic’. The study suggests an overall positive experience of patients attending the Surgical ‘Hot Clinic’. Most patients were satisfied with the service provided and preferred to attend the service instead of the Emergency Department. They would also recommend it to their family or friends. This study explores and evaluates Surgical ‘Hot Clinics’.
Patients’ overall experience of the Surgical ‘Hot Clinic’ was very good. A nurse and a surgical specialist doctor run the Surgical ‘Hot Clinic’. There is also a separate reception area with a receptionist to register the patients who attend the clinic. This allows access for quick surgical review of patients and a plan of care. The RCS recommends provision of a consultant-led service with a defined governance-led structure to deliver high quality emergency surgical service [2]. The ‘Hot Clinic’ is a step towards achieving this goal. Presence of a senior physician with a triage nurse has shown to reduce waiting times, improve patient satisfaction and effective patient flow in the Emergency Department [3 4]. A Multidisciplinary (Multispecialty) approach also helps in better streaming of patient through the Emergency Department [5]. The presence of a senior surgeon in a multidisciplinary team not only explains higher patient satisfaction rates, but also quicker patient through put. Patients also preferred this service compared to the Emergency Department, as they were seen directly by the specialist and a definitive plan of care was made at consultation. Use of Fast Track Areas in the Emergency Department has shown to reduce waiting time and length of stay in the Hospital [6]. Fast Track Areas in the Emergency Department has also shown to improve patient satisfaction [7]. Surgical ‘Hot Clinics’ also provided General Practitioners access to senior surgical doctors in managing acutely ill surgical patients. This however, has resource implications. The system could also be misused to get urgent surgical review of patients who could be seen in routine outpatient clinics, which has financial implications in a system like the NHS.
The Surgical ‘Hot Clinic’ was also situated in a clean and safe environment as confirmed by patient statements, which also adds to higher patient satisfaction.
Patients felt that they were involved in the decision-making process and that they were given adequate information regarding their illness and plan of management. Studies have shown that patients want to be involved in the decision making process [8]. Patient participation has an effect on medical decision making process, which in turn has shown to have an effect on costs and outcomes, including hospital stay [9]. This has obvious financial implications for health care provision.
Involving patients in care-related decisions is known to improve patient satisfaction rate [10].
The high satisfaction rates could be explained by the fact that most of our patients felt that they were involved in the decision making process. A health care system to serve current and future needs require new pathways with better self-management, greater transparency, improved shared decision making and innovative approaches [11]. Surgical ‘Hot Clinic’ is a new concept and in the ever-changing field of medicine, it is vital that these changes take place with the consumers (patients) at the center of decision-making. With increasing patient awareness, there is an increasing need for doctors to be trained and help patient involvement in decision-making. It is vital for a service like surgical ‘Hot Clinic’ to have patient involvement in their care.
Conclusion
Surgical hot clinics are effective alternative surgical pathways, which are well received by patients. Further research is needed to explore the patient perspectives further in the context of a NHS, which is constantly evolving to deliver better and efficient emergency surgical care.
Conflict of Interest
The authors declare that there is no conflict of interests
Authors’ contribution
VS: Protocol/project development, Data collection or management, Data analysis, Manuscript writing/editing
MI: Data collection or management
MW: Data collection or management
TA: Protocol/project development, Manuscript editing
Ethical Consideration
The study was approved by the Institute Ethics Committee.
Funding
None Declared
References
[1.Javed M, Hall B, Young S, Scarfe D, Sharma A, Ashraf S. Is “hot clinic” a “hot” idea for evaluating emergency surgical admissions? Int J Surg [Internet]. Elsevier; 2011 Jan 1 [cited 2014 Aug 16];9(7):529–30. Available from: http://www.journal-surgery.net/article/S1743919111002792/fulltext
[2].RCS TRC of S of E. Emergency Surgery: Standards for unscheduled care. 2011.
[3].Travers JP, Lee FCY. Avoiding prolonged waiting time during busy periods in the emergency department: Is there a role for the senior emergency physician in triage? Eur J Emerg Med [Internet]. 2006 Dec [cited 2014 Aug 11];13(6):342–8. Available from: http://www.ncbi.nlm.nih.gov/pubmed/17091056 [Pubmed]
[4].IMPACT on emergency department flow: improving patient processing assisted by consultant at triage. Emerg Med J [Internet]. 2004 Sep [cited 2014 Aug 4];21(5):537–41. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1726434&tool=pmcentrez&rendertype=abstract[Pubmed]
[5].Oredsson S, Jonsson H, Rognes J, Lind L, Göransson KE, Ehrenberg A, et al. A systematic review of triage-related interventions to improve patient flow in emergency departments. Scand J Trauma Resusc Emerg Med [Internet]. 2011 Jan [cited 2014 Aug 16];19:43. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3152510&tool=pmcentrez&rendertype=abstract[Pubmed]
[7].Nash K, Zachariah B, Nitschmann J, Psencik B. Evaluation of the fast track unit of a university emergency department. J Emerg Nurs [Internet]. 2007 Feb [cited 2014 Aug 6];33(1):14–20; quiz 90. Available from: http://www.sciencedirect.com/science/article/pii/S0099176706004995 [Pubmed]
[8].Guadagnoli E, Ward P. Patient participation in decision-making. Soc Sci Med [Internet]. 1998 Aug [cited 2014 Aug 16];47(3):329–39. Available from: http://www.sciencedirect.com/science/article/pii/S0277953698000598[Pubmed]
[9].Tak HJ, Ruhnke GW, Meltzer DO. Association of patient preferences for participation in decision making with length of stay and costs among hospitalized patients. JAMA Intern Med [Internet]. 2013 Jul 8 [cited 2014 Jul 24];173(13):1195–205. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23712712 [Pubmed]
[10].uh WS, Lee CK. [Impact of shared-decision making on patient satisfaction]. J Prev Med Public Health [Internet]. 2010 Jan [cited 2014 Aug 16];43(1):26–34. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20185980 [Pubmed]
[11].Sands DZ, Wald JS. Transforming health care delivery through consumer engagement, health data transparency, and patient-generated health information. Yearb Med Inform [Internet]. 2014 Jan [cited 2014 Aug 16];9(1):170–6. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25123739 [Pubmed]

