Case Report

Primary Pure Squamous Cell Carcinoma of Gallbladder: A Rare Entity
*Ram Niwas Meena, *Satyendra Kumar Tiwary, *Rahul Khanna, *Ajay K Khanna,
- *Department of Surgery, Institute of Medical Sciences, Banaras Hindu University, Varanasi 221005 India
- Submitted: Wednesday, February 18, 2015
- Accepted: Tuesday, June 02, 2015
- Published: Saturday, July 18, 2015
This is an Open Access article distributed under the terms of
the Creative Commons Attribution License
(http://creativecommons.org/licenses/by/3.0) which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Introduction
Adenocarcinoma is the most common malignant neoplasm of the gallbladder. Although areas of squamous differentiation may be seen in adenocarcinoma, primary pure squamous cell carcinoma is rarely reported and accounts for less than 1% of all gallbladder malignancies.
Case Report
We report a 50-year-old female who presented with right upper quadrant pain. She was operated on based on a presumptive diagnosis of acute cholecystitis with Empyema of gallbladder according to clinical and ultrasonographic findings. Histopathological examination revealed well differentiated keratinized squamous cell carcinoma infiltrating into the muscle layer up to the serosa. Thorough evaluations by CT scan of abdomen post operatively revealed no other primary site for the tumor.
Conclusions
Primary squamous cell carcinoma of the gallbladder is a rare histological finding. There is no consensus on its treatment due to its rarity.
Key words
Gallbladder, Squamous Cell Carcinoma, acute cholecystitis, Cholecystectomy;
Introduction
Gallbladder carcinomas are uncommon malignancies, being the fifth most common cancer of the digestive tract. It accounts for only 2% to 4% of all gastrointestinal malignancies [1]. Carcinoma of the gallbladder is more common in women and usually seen in patients older than 50 years of age.
Adenocarcinoma is the most common malignant neoplasm of the gallbladder [2]. Although area of squamous differentiation is seen in adenocarcinoma, pure primary squamous cell carcinoma is rarely reported and accounts for less than 1% of all gallbladder malignancies [2]. We report a case of pure squamous cell carcinoma of gallbladder which is rare histology finding.
Case Report
A 50-year-old female presented at the outpatient department of surgery with complaints of pain in right hypochondrium and dyspepsia for 2 months and there is no history of jaundice, loss of weight and appetite. It was associated with nausea, vomiting and mild grade fever from 1week. Physical examination revealed the presence of tenderness in right hypochondrium but no palpable lump and organomegaly was observed. She was febrile with an orally obtained temperature of 38.5°C. Blood investigation showed only leukocytosis, renal function, and liver function was absolutely normal.
USG abdomen revealed distended gallbladder with thickened wall of 7mm and suspicious hyperechoic mass measuring 4 × 2 cm with having debris and stone in gallbladder. On this basis, a clinical diagnosis of acute calculus cholecystitis with Empyema of gallbladder was considered. Patient was admitted in surgery ward and received supportive care and antibiotics. Despite of this treatment no improvement, so planned emergency cholecystectomy. She finally underwent open cholecystectomy.
Operative finding of the gallbladder revealed an ill-defined infiltrating creamy white friable mass in the body of the gallbladder measuring 3×2 cm size, filled with multiple stone inside with adhesions to the omentum, possibly carcinoma. No obvious involvement of liver, cystic duct, common bile duct, hepatic flexure was observed (Figure 1). Post-operative course was uneventful.

Figure 1 Cut opened specimen of gall bladder shows a 4 x 2 cm irregular grey –white friable mass in gall bladder lumen with stone.
Histopathological examination showed well differentiated keratinized squamous cell carcinoma of the gallbladder infiltrating into the muscle layer up to the serosa. The keratinization was extensive with numerous keratin pearls and dyskeratotic cells (Figure.2 & 3). In the follow-up visits patients received six cycles of chemotherapy (gemcitabine 100mg/m2 and oxaliplatin 100mg/m2) and the patient was well in a follow-up period of 6 months and no loco-regional recurrence seen in CT scan of abdomen.
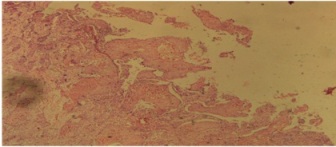
Figure 2: Microscopic examination show well differentiated keratinize squamous cell carcinoma of gallbladder infiltrated up to serosa a characterize by keratin pearls (10x)
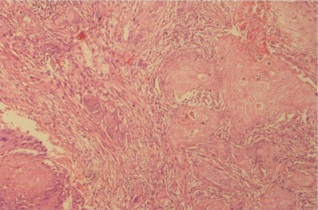
Figure 3: Microscopic examination show well differentiated keratinized squamous cell carcinoma of gall bladder of gallbladder infiltrated up to serose characterized by keratin pearls and intercellular bridges (40x)
Discussion
North India is one of the regions having highest incidence of gallbladder carcinoma. Other high incidence areas are reported in Latin America and Eastern Europe. It shows female preponderance with F: M ratio of 3–4: 1. Gallbladder cancer commonly presents between the 4th and 6th decades of life [3], while our patient was 50 year old female.
Gallbladder cancer is an uncommon and aggressive malignancy, and a high proportion of patients have advanced-stage disease at presentation [4]. Adenocarcinoma is the most common histological subtype of gallbladder cancer constituting about 90-95% of the cases. Although areas of squamous differentiation are seen in some reported cases, pure squamous cell carcinoma of the gallbladder is very rare [2].
Pure squamous cell carcinoma of the gallbladder grows slowly, is usually localized and rarely metastasized, It is a highly malignant neoplasm presenting at an advanced stage in majority of the cases. Surgery is the only treatment available, only when diagnosed at an early stage.
Etiology for squamous cell carcinoma in the gallbladder is not well defined. Epithelial tumor genesis is a multistep process resulting from sequential genetic alteration at different stages of evolution. Because a normal gallbladder has no squamous epithelium, the source of origin is questionable. The most plausible theory involves squamous metaplasia or squamous differentiation of adenocarcinoma. According to this hypothesis, squamous cell carcinoma of gallbladder develops as follows. An initial pre-existing adenocarcinoma that undergoes squamous metaplasia to produce adenosquamous carcinoma and this metaplastic carcinoma subsequently grows rapidly and replaces the adenocarcinoma component to form pure squamous cell carcinoma. [5]
In our case squamous cell carcinoma infiltrated into the muscle layer up to the serosa from the mucosal surface and it was found not to contain either a part of an adenocarcinoma or the transitional cells of adenocarcinoma in conversion to squamous cell carcinoma.
Gall stones appear to be a major risk factor in the carcinogenesis of carcinoma of any type but more so for squamous cell carcinoma. Approximately 90% of squamous cell carcinoma cases invariably have cholelithiasis. [6], as our case also revealed gall stones.
Kumar et al., [7] claim that the pure squamous cell carcinoma is characterized by a well-localized growth with no lymph nodal or visceral metastasis, even with tumors of large size. Radical resection is the mainstay of treatment for patients with locally invasive squamous cell carcinoma and offers the only chance for cure. Laparoscopy should not be done if gallbladder cancer is suspected. If during initial laparoscopy the diagnosis is suspected, conversion to an open laparotomy should en-sue to maximize potential for a curative resection [8]. Laparoscopy has been shown to be an important staging tool in the management of gastrointestinal malignancies because it provides the ability to identify radiographically occult disseminated disease before proceeding to laparotomy for an attempt at resection [9].
Postoperative radiotherapy and chemotherapy may be used however results are inconsistent [10], but in our case we used Gemox regimen as chemotherapy may be of benefit to patient.
Conclusion
Pure primary squamous cell carcinoma of the gallbladder is rarely reported, diagnosis is only after surgery. So, histopathologist should be careful always in cases of acute cholecystitis and by expert pathologist correct diagnosis can be made. Radical resection is the mainstay of treatment for locally invasive squamous cell carcinoma and offers a chance of cure in early stage of disease. Role of chemotherapy as adjuvant therapy is not defined well till now.
Authors' Contribution
RNM: Did the literature search and prepared the draft manuscript
SKT: Helped in preparation of draft manuscript
RK: Helped in acquisition of data and analysis
AKK: Conceived and designed the study and edited the final version
Conflict of Interests
The authors declare that there is no conflicts of interests
Ethical Considerations
Written informed consent was obtained from the patient for publication of this case report.
Funding
None declared
Acknowledgement
None
References
[1].Kumar V, Cotran RS, Robbins SL. Robbins basic pathology. 7thed, Philadelphia: WB Saunders; 2003.
[2].Roa JC, Tapia O, Cakir A, Basturk O,Dursun N, Akdemir D, et al. Squamous celland adenosquamous carcinomas of the gallbladder: clinicopathological analysis of 34 cases identified in 606 carcinomas. Mod Pathol. 2011; 24:1069-78[PubMed]
[3].Waisberg J, Bromberg SH, Franco MI, Yamagushi N, dos Santos PA, Castro MA. Squamous Cell Carcinoma of the Gallbladder. Sao Paulo Med J. 2001 Jan 4; 119(1):43 [PubMed]
[4].Butte JM, Matsuo K, Gonen M, D'Angelica MI, Waugh E, Allen PJ, Fong Y, DeMatteo RP, Blumgart L, Endo I, De La Fuente H, Jarnagin WR. Gallbladder cancer: differences in presentation, surgical treatment, and survival in patients treated at centres in three countries. J Am Coll Surg. 2011; 212:50–61 [PubMed]
[5].Roppongi T, Takeyoshi I, Ohwada S, Sato Y, Fujii T, Honma M, Morishita Y. Minute squamous cell carcinoma of gallbladder: A case report. Jpn J Clin Oncol. 2000 Jan; 30(1): 43-5 [PubMed]
[6].Schwrtz SL, Shires E, Spencer FC, Daly JM, Fisher JE, Galloway AC. Principles of surgery. 7th ed, New York: McGraw-Hill; 2006
[7].Kumar A, Singh MK, Kapur BM. Synchronous double malignant tumors of the gallbladder: A case report of Squamous cell carcinoma and angiosarcoma. Eur J Surg Oncol 1994; 20:63-7 [PubMed]
[8].Memon MA, Anwar S, Shiwani MH, Memon B. Gallbladder carcinoma: a retrospective analysis of twenty-two years experience of a single teaching hospital. Int Semin Surg Oncol. 2005 Mar 17;2(1):6. [PubMed]
[9].Chang L, Stefanidis D, Richardson WS, Earle DB, Fanelli RD. The role of staging laparoscopy for intra-abdominal cancers: an evidence-based review. Surg Endosc. 2009; 23:231–241 [Pubmed]
[10].D’Angelica M and Jarnagin W. “Tumors of the Gallbladder,” In Blumgart LH, Ed., Surgery of the Liver, Biliary Tract, and Pancreas, 4th Edition, WB Saunders, Amsterdam, 2006, pp. 764-781.

