Case Report

Necrotic Pseudoxanthomatous Nodule: An Unusual and Less Known Manifestation of Endometriosis
* Kiran Agarwal, *Deepti Verma, *Anamika Kashyap *, Archna
Rautela
- *Department of Pathology, Lady Hardinge Medical College, Delhi, India
- Submitted: Wednesday, May 14, 2014
- Accepted:Wednesday, July 09, 2014
- Published: Wednesday, October 22, 2014
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Abstract
Necrotic pseudoxanthomatous nodule (NPN) is an uncommon manifestation of endometriosis. It grossly presents as nodules over peritoneal surfaces. Histopathologically, it is marked by presence of a central area of necrosis surrounded by hyalinization and histiocytes arranged in a palisaded fashion along the periphery of the necrotic area. These histiocytes have abundant granular or foamy cytoplasm. It represents the end stage endometriosis. Here we are reporting two such cases. It is important to know about this entity as it can be confused with necrotic tumor or infectious pathology, to avoid misdiagnosis in the absence of more classical features of endometriosis and from management point of view.
Keywords
necrotic pseudoxanthomatous nodule, endometriosis, necrosis, histiocytes
Introduction
Endometriosis is an important cause of infertility. Its recognition depends upon the presence of endometriotic glands and stroma in aberrant sites. Necrotic pseudoxanthomatous nodule (NPN) is an unusual manifestation of endometriosis which tends to occur in postmenopausal and late reproductive age groups [1]. It is important to know and identify this entity to avoid confusion from carcinoma. We are reporting two such cases.
Case 1
A 24 years old female presented to gynecologicaloutpatient department with primary infertility for four years. She was on ovulation induction therapy for the past two years but she failed to conceive. Hysterosalpingography showed bilateral cornual block with absence of free peritoneal spill. Diagnostic laparoscopy thereby performed showed presence of adhesions between ovary, fallopian tube and omentum. Few nodules were found over the ovarian surface which werebiopsied and sent for the histopathological examination.
Case2
A 35 years old female presented to gynecological outpatient department with complaints of secondary infertility for 5 years. Hysterosalpingography showed right peritoneal spill with left tubal block. Laparotomy showed dense adhesions between the left fallopian tube, ovary and intestine along with left endometrioma along with small nodules over the surface of left fallopian tube. Biopsy from the left endometriotic cyst and nodules over the left fallopian tube were sent for histopathological examination.
Microscopic examination of the nodular biopsy tissue from both the cases showed similar picture. A central area of necrosis was identified surrounded by histiocytes and hyalinisation. These histiocytes had abundant foamy cytoplasm and were arranged in apalisaded fashion along the periphery of the necrotic area (Figure 1 and
2). The endometriotic glands and stroma were absent. The second case also showed presence of endometrial glands and stromain the biopsy tissue from the endometriotic cyst( Figure 2
lower inset) ). The PAS stain in both the cases showed positivity in the histiocytes. Based on the above features, the diagnosis of NPN was given in both the cases.
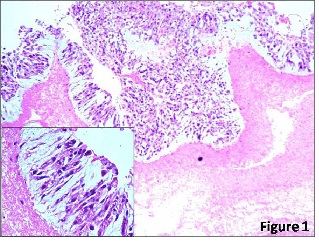
Figure 1: The biopsy from the first case showing a central area of necrosis surrounded by the histiocytes in a palisaded fashion (H/E,
x100). Lower inset shows histiocytes with foamy cytoplasm (H/E, x400).
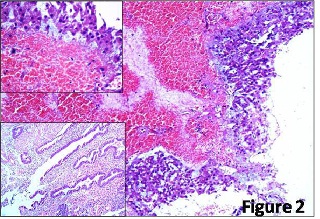
Figure 2: The biopsy of the fallopian tube from the second case showing a central area of hemorrhage and necrosis surrounded by the histiocytes in a paliasaded fashion (H/E, 100). The upper inset shows the histiocytes under higher magnification (H/E,
x400) with granular cytoplasm. The lower inset shows the presence of endometrial glands and stroma in the biopsy tissue from endometriotic cyst (H/E,
x100).
The histopathological diagnosis of endometriosis is based upon the recognition of endometriotic glands and stroma in ovarian and extra ovarian sites. However, several unusual aspects may raise the concern for a neoplasm, including atypical endometriosis, mass forming lesions, polypoidal growth, lymphovascular or perineural involvement and NPN [2].
The NPN represents the end stage endometriotic foci [2 3] and is seen as multiple nodules that are usually attached to peritoneum or occasionally freely floating in the peritoneal cavity. These can be confused intraoperatively with disseminated malignant tumor [1]. Microscopically, these comprise up of central area of necrosis surrounded by histiocytes and hyalinization. The histiocytes have abundant foamy or granular cytoplasm hence the term pseudoxanthomatous. More typical foci of endometriosis are not usually found adjacent to these areas but often in other sites in the same patient. Similar findings were present in our case on the basis of which the diagnosis of NPN was made.
Due to presence of necrosis this entity can be confused with necrotic tumor or infectious pathology, necrotic peritoneal and ovarian granulomas[1 2 3 4]. Thus awareness of this etiology is important to avoid unnecessary investigations.
Clement P B et al., [4]reported four cases of NPN in which the diagnostic endometriotic glands and stroma were typically absent in nodules and their immediate vicinity. However, foci of recognizable endometriosis were found in the ovaries in all cases. In one of the case, several necrotic nodules were found to line an endometriotic cyst.
Carey et al.,[5] described a case of 39 years oldwoman who presented with acute abdominal pain and an abdominopelvic mass which was discovered to be a large endometrioma with an associated endometrioid adenocarcinoma.Subsequently seven weeks later, multiple NPN of the peritoneal and omentum were found on surgical exploration. It was then concluded that pseudoxanthomatous nodules of peritoneum and omentum may arise from a peculiar reaction to endometriotic cyst contents and clinically can mimic metastatic ovarian carcinoma.
To conclude, it is important to know NPN as an unusual feature of endometriosis; it’s significance rests on it being diagnostic or at least strongly suggestive of endometriosis when more typical features of endometriosis like endometrial glands and stromaare absent and not miss the diagnosis of endometriosis.Also it’s important not to misinterpret NPN as necrotic tumor or infectious pathology and thus avoid unnecessary investigations.
Authors’ Contribution
KA: Analysis, interpretation of data and editing.
DV: Literature search and manuscript draft.
AK: Collection of data and contribution to clinico-pathological part of manuscript.
AR: Analysis and interpretation of results and preparation of draft.
Ethical Considerations
Written informed consent was obtained from both the patients for publication of this case report.
Conflict of Interests
The authors declare that there are no conflicts of interests.
Acknowledgement
None declared
Funding
None declared
References
[1].Clement P B. The Pathology of Endometriosis A Survey of the Many Faces of a Common Disease Emphasizing Diagnostic Pitfalls and Unusual and Newly Appreciated Aspects. AdvAnatPathol2007; 14: 241-260 [Pubmed]
[2].Medeiros F, Bell D A. Pseudoneoplastic Lesions of the Female Genital Tract. Arch Pathol Lab Med 2010; 134: 393-403. [Pubmed]
[3].Clements P B. Selected miscellaneous ovarian lesions: small cell carcinomas, mesothelial lesions, mesenchymal and mixed neoplasms, and non-neoplastic lesions. Modern Pathology 2005; 18: S113-S129.
[4].Clement PB, Young RH, Scully RE. Necrotic pseudoxanthomatous nodules of ovary and peritoneum in endometriosis. AJSP1988; 12 (5): 390-7 [Pubmed]
[5].Carey M, Kirk ME. Necrotic pseudoxanthomatous nodules of the omentum and peritoneum: a peculiar reaction to endometriotic cyst contents. ObstretGynecol 1993; 82(4 part 2): 650-2[Pubmed]

